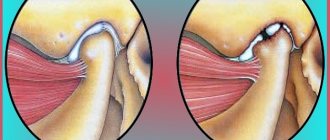
Main types of jaw cysts
The tumor can appear on both the upper and lower jaw
The main types of cysts are presented in the table.
Table 1. Classification of jaw cysts:
| Type of cyst | Description |
| Keratocyst of the mandible | The most common type of cyst. Formed in the area of 3 molars. It can be single-chamber or multi-chamber. |
| Radicular | This type of neoplasm accounts for 82% of all cysts. The size varies from 0.6 to 2 cm. |
| Follicular cyst of the lower jaw | Also called an unerupted tooth cyst. Located in the alveolar edge of the jaws. |
| Retromolar | Occurs against the background of problematic teething. |
| Cholesteatoma | It is a tumor-like cyst-like neoplasm. Its shell is covered with epidermis. |
| Aneurysmal | Occurs infrequently. The etiology of the neoplasm has not been sufficiently studied. |
| Traumatic | Non-epithelial neoplasm. It is rare and occurs on the lower jaw. |
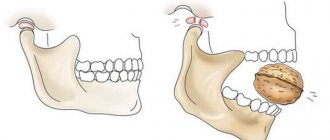
Reasons for appearance
The following factors for the development of jaw cysts are identified:
- gum injury;
- penetration of infection into the dental tubules;
- tooth injury;
- sinusitis and other ENT pathologies;
- incorrect tooth development.
Varieties
Jaw cysts are divided into several types. They are classified depending on their location, mechanism of occurrence and structure.
Primordial
Their second name is keratocysts. They form in the area of the third molars (chewing teeth) or in the corner of the lower jaw. Sometimes capsules may appear in place of the missing unit. Both single and multiple formations are noted. The latter are often multi-chamber.
A jaw cyst is a benign formation.
This species consists of thin fibrous tissue and odontogenic epithelium. It recurs frequently.
Follicular
Such neoplasms are also called “cysts of unerupted teeth,” which explains the mechanism of their appearance: they are formed in the place of ungrown or partially emerged units. The capsules are localized in the area of the fangs, 2nd and 3rd molars, and the alveolar process of the jaw. They are covered with flat multilayered epithelium, which often becomes denser. Mucus formation may occur.
Radicular
The most common type - occurs in almost 80% of patients. Formations most often appear on the upper jaw (up to 70%). Their size is 0.5 – 2 cm in diameter, but sometimes it exceeds 3 cm.
Radicular capsules often become inflamed and suppurate. They are characterized by the appearance of network-like processes penetrating into the thickness of the wall. They can be located in the area of any teeth. Large conglomerates lead to destructive lesions of bone tissue.
Important! Radicular cysts are often located next to the maxillary sinuses or penetrate into them. This contributes to the development of sinusitis.
Retromolar
Cysts are divided into several types.
Another type of eruption cyst. However, it develops with chronic periodontal inflammation that accompanies the appearance of teeth.
Associated symptoms
At the initial stage, the growth of the cyst is not accompanied by specific symptoms. Characteristic signs appear against the background of transformation of the neoplasm. The table presents the main symptoms of a mandibular cyst.
Table 2. Signs of cyst transformation:
| Sign | Description |
| Can be very strong. Appears at the site of bone damage. The pain is constantly getting worse. |
| In difficult cases it rises to 39-40 degrees. |
| The appetite disappears, the person feels weak. |
| May transform into vomiting. |
| It is constantly increasing. |
Note! Such symptoms indicate the beginning of the process of suppuration. Treatment must be immediate.
Symptoms and complications
In the initial stages, the disease does not manifest itself. The patient has no complaints of discomfort or other subjective sensations. As the jaw cyst develops, symptoms :
- A protruding, painless formation inside the oral cavity.
- Severe pain during chewing and hyperemia of the mucous membranes during the purulent course of the disease.
- Swelling of the gums.
Important! The formations may periodically open up on their own. In this case, there is an outflow of exudate through the fistula, sometimes the contents are poured into the maxillary sinuses. After a while, the capsules are filled with liquid again.
Cysts are benign formations. However, they can lead to significant complications :
- loss of one or more teeth;
- periostitis - inflammation of the periosteum;
- osteomyelitis – purulent lesion of bone tissue;
- sinusitis;
- pathological fracture of the jaw;
- sepsis - penetration of purulent contents into the bloodstream.
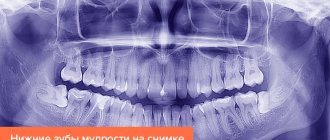
The main way to detect the disease and its type is radiographic.
Types of salivary gland cysts
The appearance of pathological cavities is due to partial or complete inhibition of secretory outflow. The main types of salivary gland cysts are presented in the table.
Table 3. Types of salivary gland cysts:
| View | Subspecies | Symptoms |
| Molar, lingual, palatal, buccal, labial. | There is discomfort when eating. Sometimes unpleasant sensations appear during sleep. Against the background of trauma to the neoplasm, a yellowish discharge of a viscous consistency appears. |
| Ranula, parotid, submandibular salivary gland cyst. | Facial asymmetry, formation of new skin folds. A submandibular cyst is characterized by the appearance of a painless swelling. |
Establishing a diagnosis
To clarify the diagnosis, the doctor refers the patient for a comprehensive examination. The main research methods are presented in the table.
Table 4. Diagnostic methods:
| Method | Target | Description |
| Determining the location of the tumor. | On an x-ray, the neoplasm appears as an oval-shaped shadow. It has clear boundaries. The image shows the extent of destruction of the bone structure. |
| Obtaining more detailed information about the cyst. | It is carried out against the background of the impossibility of differentiating the tumor in the image. |
| Determination of the nature of the neoplasm. | The main indication is a cyst of the intramaxillary sinus. The procedure is carried out to exclude the malignancy of the tumor component. |
Diagnosis and treatment
The main way to detect the disease and its type is radiographic. Applicable:
- targeted images (film or performed by a radiophysiographer) – capture the area from 1 to 4 teeth;
- orthopantogram or panoramic photographs - give a complete picture of the structure of the jaw system, help to identify the extent and depth of the lesion;
- MRI – during the study, the skull is scanned with multiple images in different planes.
An informative diagnostic method is a panoramic image.
Important! On the x-ray, cavities with clear contours will be visible. If a capsule of the follicular or retromolar type has formed, the image will show unerupted teeth embedded in the bone.
If a cyst occurs on the jaw, treatment is carried out surgically followed by therapy. Two types of surgery are used: cystectomy and cystotomy.
Cystectomy
It involves complete removal of the capsule, filling the cavity with biocomposite materials and suturing the wound. The factors for its purpose are:
- Small formations located within 1 – 2 teeth. Their roots should be immersed in the capsule no more than a third of their length.
- Extensive cyst of the lower or upper jaw.
If a cyst occurs on the jaw, treatment is carried out surgically followed by therapy.
The disadvantage of cystectomy is the frequent infection of the wound and, as a consequence, recurrence of the formation. Damage to intact (adjacent) units, the pulp (neurovascular bundle), and the maxillary or nasal sinuses is also possible.
Basic treatment methods
Specific treatment is required when the condition of the tumor changes
If the cyst in the jaw is 1 to 3 mm in size, then the therapeutic tactic is to monitor it.
If her condition changes, then treatment is as follows:
- Rinse the root tubules . The specialist injects potent medications into the affected area. Then the tissue is cemented.
- Surgical intervention . The type of surgery depends on the type of cyst.
- Conducting antibacterial therapy . Antibiotics are prescribed during an acute purulent process. Medicines are administered by injection.
Note! Procedures for washing and cementing tissue are carried out only for radicular cysts.
Therapy
In cases where the formation is small in size (up to 3 mm), it is called granuloma. For some time, such formations should be under the supervision of a doctor. Treatment of a mandibular cyst is indicated only if the granuloma begins to increase in size. The main methods of treating cystic formations are the following.
- Therapeutic manipulations. Specialists prescribe rinsing of the root canals, into which medications are then injected, and tissue cementation. Under the influence of drugs, the cystic formation thickens and is neutralized. Therapeutic treatment can only be used in cases where the cyst has a radicular shape and a size of no more than 0.8 cm.
- All other methods involve surgery. Cystectomy is an operation to remove the infectious focus and adjacent tissues that have been affected.
- Cystotomy is the most popular method of removing a mandibular cyst, which allows you to save the tooth. With cystomy, the anterior wall of the tumor is removed and all pathological contents are scraped out.
- Plastic cystectomy is a procedure similar to simple cystectomy. The main difference is that the soft tissues are not sutured after removal of the tumor. This method of surgical intervention is used, as a rule, in advanced conditions accompanied by complications.
- Two-phase surgery for mandibular cyst. It is a more complex procedure, which is prescribed exclusively in the most difficult cases. During the operation, the surgeon tries to preserve intact teeth and tissues as much as possible, while removing the infectious focus. A two-phase operation includes cystectomy and cystomy, which are performed in a specific order.
- Removal of the cyst along with the tooth. This method is used mainly when the cyst is localized in the area of the eighth molar.
- If the pathology leads to the development of osteomyelitis, the patient is shown a more serious intervention, in which the infected area is opened and the destroyed tissue and pus are carefully scraped out.
Surgery
The main types of surgical intervention are presented in the table.
Table 5. Types of surgical treatment:
| Type of surgery | Purpose of the operation | Description |
| Removal of the infectious focus and affected roots. An operation is performed when a cyst on the lower jaw involves 2 teeth. | During the operation, the surgeon removes the cavity, the affected part of the root and the membrane. The final stage of the operation is drying. |
| Creation of a zone from the cyst that can communicate with the oral cavity. The main indication is an extensive cyst of the lower jaw. | During surgery, the doctor removes the anterior wall of the cystic formation. Surgery involves severe destruction of the nasal bone floor and the plate of the palate. The rehabilitation period is characterized by duration. |
| Prescribed for severe cases and complications. | The surgery is performed in much the same way as a regular cystectomy. There is no suturing of soft tissues. |
| The main task is to preserve healthy teeth or their fragments. This is a very complex surgical intervention, performed only in advanced cases. | During the operation, the surgeon combines the methods of cystectomy and cystotomy. This approach allows you to completely remove the infectious focus and injure the tissue to a lesser extent. |
Note! Sometimes the surgeon removes the damaged tooth along with the cyst. This operation is performed if the jaw cyst is located next to the wisdom tooth.
Surgical treatment of minor salivary glands
The instructions for the doctor are as follows:
- Infiltration anesthesia. The pain impulse is blocked in the sensitive receptor area.
- Improving access to the cyst. This avoids severe blood loss.
- Removal of the tumor. 2 small incisions are made over the cyst.
- Removal of damaged lobules of the minor salivary gland.
- Stitching. They are layer by layer.
- Applying a compression bandage.
The duration of the operation depends on the type of cyst. Patients usually tolerate surgery well.
Other types of surgery
The table shows other types of surgical interventions.
Table 6. Other methods of operation:
| Type of cyst | Operation | Description |
| Cystsialadenectomy | The specialist removes both the tumor itself and the salivary gland. |
| Parotidectomy | Surgery is prescribed when there is a risk of infectious relapse. If the cyst is located above the facial nerve, superficial surgery is performed. |
| At the discretion of the doctor | Both the cyst under the jaw and the gland are removed. This avoids the risk of relapse. |
If the growth of the cyst has led to the initial stage of osteomyelitis, the surgeon undertakes to open the affected area. The cavity is carefully scraped out.
This procedure involves removing pus and tissue that has been destroyed. After this, the patient is prescribed antibiotics.
Postoperative period
The duration of the postoperative period varies from 5 to 14 days
The plate provides information about returning to work after surgery.
Table 7. Return to work capacity:
| Features of the cyst | Type of surgery | Recovery time |
| Small and medium tumor size | Cystectomy | 5-7 days. After surgery, a small hematoma may appear. The overall temperature rises slightly. |
| Large tumor size | Cystotomy | 14 days. |
| Granuloma | Cystectomy | 5-14 days. |
| Symmetrical fibroma of the maxilla | Cystectomy | 8-10 days. |
Oral care after surgery should be thorough. The operated area and surrounding tissues should be treated with a piece of gauze soaked in a 5% hydrogen peroxide solution. This should be done after every meal and before going to bed.
After parotidectomy, stitches are placed. When they are removed, the operated area should be cleaned with mild soap and water.
Note! After surgery, you should not take aspirin. This drug causes bleeding.
If pain and swelling persist for longer than 2 weeks, you should contact the doctor performing the surgery again.
NONODONTOGENIC JAW CYSTS
Pathogenetically,
non-odontogenic cysts of the jaws are not associated either with teeth or with a disorder in the development of the dental epithelium. Their occurrence is associated with a violation of facial embryogenesis (embryonic dysplasia). These are so-called fissural (cleft) cysts. They develop in the embryonic period at the border of the embryonic facial processes. Localized on the upper jaw, they are rare (according to our data, in 2% of cases). Depending on the location, the following fissural cysts are distinguished: nasopalatine, globulomaxillary
and
nasoalveolar.
Nasopalatine cysts (incisive canal cysts) develop from the embryonic remains of the epithelium of the nasopalatine canal. The nasopalatine canal is an epithelialized
“tube” located in the bone incisive canal. The latter connects the bottom of the nasal cavity and the oral cavity. Cysts can occur in any part of this canal, but much more often they form in its lower parts.
Depending on the location of the development of the cyst, its pathological
structure. In the upper part of the canal (closer to the nasal cavity), the cysts are lined with columnar or ciliated epithelium, in the lower parts - with multilayered squamous epithelium.
Rice. 27.5.1. Radiographs of the upper jaw of patients with nasopalatine
(incisive canal) cysts (a, b, c).
Nasopalatine cysts are located between the central incisors. The growth of the cyst is slow and painless. After destruction of the palatine bone, a hemispherical protrusion with clear boundaries appears in the anterior part of the palate, behind the intact central incisors. When punctured, you can get a clear liquid with cholesterol crystals. Cysts may fester.
27. JAW CYSTS
Diagnosis
established on the basis of x-ray examination.
In the area where the incisive opening should be located, there is a focus of homogeneous rarefaction of bone tissue with clear boundaries {Fig.
27.5.1). This lesion has a round shape and is located strictly along the midline.
Intact tooth roots are projected onto it, preserving the periodontal fissure. Errors
in making a diagnosis occur in the presence of destroyed upper central incisors. On an x-ray, it is necessary to determine whether there is destruction of the periodontal fissure of the tooth, which is projected onto the cyst. The latter indicates an existing radicular cyst. The final diagnosis is established after pathohistological examination.
Globulomaxillary cysts (intramaxillary, spherical-maxillary) are located between the lateral incisor and the canine on the upper jaw. Formed from the epithelium at the site of fusion of two embryonic facial processes: frontal (processus globulahs)
and maxillary
{processus maxillaris).
These are nonodontogenic epithelial cysts of the jaw bones. Their shell is thin and lined with flat, cubic or columnar epithelium.
Cysts grow slowly and painlessly. They are often discovered by accident. Clinically, they manifest themselves as a painless protrusion in the vestibule of the oral cavity or palate. They can grow into the nasal cavity or maxillary sinus. The cyst is located in the area of intact teeth. Suppuration of cysts is rare. During puncture, you can obtain a clear liquid with cholesterol crystals.
On the intraoral radiograph there is an area of homogeneous rarefaction of bone tissue of a round shape with clear boundaries. The cyst is located between the intact lateral incisor and the canine (Fig. 27.5.2).
69 0
V)
G)
Rice. 27.5.2. Radiographs of the upper jaw of patients with globulomaxillary cysts (a, b, c, d).
27.5. NON-ODONTOGENIC CYSTS OF THE JAWS
Divergence (divergence) of the roots of these teeth is noted, the periodontal fissure is preserved. The diagnosis becomes more complicated if the lateral incisor or canine is destroyed (periodontitis).
Nasoalveolar cysts (nasolabial cysts of the nasal vestibule) develop from the remains of the embryonic epithelium at the border of three embryonic processes: frontal, external nasal and maxillary. The cyst is lined with a membrane covered with flat, cubic, transitional or ciliated epithelium. They are located in the area of the nasolabial furrow under the base of the wing of the nose.
Nasoalveolar cysts are located on the anterior wall of the maxillary bone in the vestibule of the oral cavity, in the projection of the roots of the lateral incisor and canine. They cause deformation (indentation) of the outer cortical plate. In the area of the nasolabial groove under the base of the wing of the nose, there is a sedentary, elastic protrusion of a round shape with clear boundaries and not fused with the surrounding tissues. There may be a narrowing of the entrance to the nose. These cysts, localized on the maxillary bone, are located in the thickness of the soft tissues. When punctured, you can get a clear, yellowish, somewhat viscous liquid with cholesterol crystals. X-ray
the cyst does not manifest itself in any way; in some cases, there may be a small rounded clearing (due to deepening) of the bone tissue at the location of the cyst.
The teeth located in the cyst area are intact. The diagnosis is clarified
during surgery.
TREATMENT OF JAW CYSTS
Jaw cysts are treated surgically. There are two main surgical methods: cystectomy
and
cystotomy.
Cystectomy is a radical surgical treatment method, which consists of completely removing the cyst shell, followed by tightly suturing the surgical wound (applying a primary blind suture to the wound).
Cystotomy is a method of surgical treatment in which the outer (front) wall of the cyst is removed along with the adjacent bone and the existing intraosseous cavity is connected to the vestibule of the mouth, i.e. the cystic cavity is turned into an additional bay of the oral cavity.
Indications for istectomy
are odontogenic and non-odontogenic cysts of the jaws at any age.
Indications for istotomy
can be:
1. large cysts of the upper jaw, which grow into the maxillary sinus with destruction of the bone floor of the nasal cavity and palatine plate;
2. extensive cysts of the lower jaw with significant thinning of the bone walls of the jaw (in the event that complete removal of the cyst shell can significantly weaken the strength of the jaw and contribute to the occurrence of a pathological fracture);
3. the patient’s old age or the presence of severe concomitant diseases (cardiovascular, endocrine, cachexia, etc.);
4. hematological diseases (hemorrhagic diathesis, hemophilia, etc.);
5. in a mixed dentition, if an attempt to completely remove the cyst shell may damage the rudiments of permanent teeth, which will affect the formation of a normal occlusion.
The advantage of an istectomy
It must be assumed that the entire cyst shell is removed, which is subjected to pathomorphological examination, and reparative bone regeneration occurs in the resulting bone cavity, because The postoperative wound is sutured tightly.
Disadvantages and istectomies:
traumatic operation; the possibility of damage to nearby intact teeth; injury to the neurovascular bundle; the likelihood of opening the walls of the maxillary sinus or nasal cavity; the possibility of autolysis (decomposition) of a blood clot located in the bone cavity cannot be ruled out.
Advantages and istotomies:
low morbidity; the operation is easy to perform; There is no danger of damage to the follicles of permanent or intact teeth, as well as surrounding bone structures, cavities and neurovascular trunks.
Disadvantages and istotomies:
non-radicality of surgical intervention; the formation of additional bays (cavities) that require long-term postoperative care; the presence of postoperative jaw deformities; the resulting open postoperative jaw defects impair the cleansing of the oral cavity with oral fluid, which creates conditions for the proliferation of microorganisms.
Cystectomy surgery technique. Surgery is performed under local anesthesia. A trapezoidal (in the anterior) or angular (in the lateral) incision is made on the vestibular surface of the alveolar process of the jaw. A horizontal incision of the mucosa is made along the crest of the alveolar process in the absence of teeth or along the neck of the teeth. The incision is made down to the bone. Lateral incisions of soft tissues for peeling off the mucoperiosteal flap must be made so that they pass along
691
27. JAW CYSTS
healthy bones, i.e. at a distance of at least 1 cm from the radiographic boundaries of the cyst. This should be done so that the suture lines do not coincide with the bone defect, which leads to the formation of fistulas leading into the postoperative bone cavity. The mucoperiosteal flap is peeled off with a rasp. Next, trepanation of the bone or expansion of the existing burr hole begins (Fig. 27.6.1).
Rice. 27.6.1. Stages of cystectomy: a - detachment of the mucoperiosteal flap, 6 - appearance of the bone wound after removal of the cystic membrane.
Fig.27.6.2. Radiographs of the lower jaw of a patient with a radicular cyst, and -before
Postoperative complications
The risk of complications arises due to the removal of the salivary gland. This is due to the possible connection of the neoplasm with the branches of the facial nerve.
Violation of its integrity leads to cessation of the functioning of facial muscles. As a result, the face is distorted.
After parotidectomy
The most serious complication after parotidectomy is airway swelling
After such surgery, the following complications may develop:
- numbness of the face;
- damage to the nerves that control the movements of the facial muscles;
- numbness of the ear;
- salivary drainage;
- Frey syndrome;
- the appearance of fistulas;
- swelling of the airways.
Older patients, people who smoke, people with diabetes and those with high blood pressure are at risk of heart attack. This can happen both during surgery and after it.
In order to prevent dangerous complications, you need to inform your doctor in detail about your health status.
After surgery on the upper jaw
Common complications are presented in the table.
Table 8. Complications after surgery on the upper jaw:
| Type of complication | Description |
| Formed against the background of injury to a large vessel. |
| Possible during cystectomy. To prevent this risk, the surgeon uses a periodontal splint. If the injury occurred during surgery, the specialist immobilizes the jaw. |
| This is possible against the background of the development of an odontogenic neoplasm in the premolar or molar zone. |
Home treatment
Further treatment is carried out at home. The main methods of “home” therapy include:
- use of folk remedies;
- oral care;
- compliance with dietary recommendations.
Folk remedies are used only under the supervision of a doctor.
The use of folk remedies
The most effective recipes are presented in the table.
Table 9. Treatment with folk remedies:
| Means | Preparation | Number of procedures |
| Pour 2 tablespoons of 200 ml of warm boiled water. Mix thoroughly and use for mouth rinsing. | 3-4 times/24 hours. |
| 1 tablespoon of herb is poured into 180 ml of liquid just removed from the stove, infused for 120 minutes. Then the broth is filtered, cooled to room temperature and used for rinsing. | 2-3 times/24 hours. |
| 0.5 tsp dissolve in 170 ml of warm boiled water. Add 0.5 tsp of iodized salt and mix thoroughly. The solution is used for baths and rinses. | Every 3 hours. |
| Pour 5 tablespoons of fresh needles into 1000 ml of boiling liquid. Cook for 30 minutes, cool, filter. The decoction is taken orally. | 2 times/24 hours. |
Note! These products can be used for compresses.
Dietary recommendations
It is recommended to diversify your diet with foods that contain vitamins and minerals. Particular attention should be paid to foods containing fluoride and calcium. You should also eat foods that stimulate saliva production.
Table 10. Dietary recommendations:
| Product | How best to use | Daily serving size (grams) |
| It is recommended to drink freshly squeezed juices. It is acceptable to add a small amount of sugar. | 150-170 ml. |
| Preference should be given to sour green varieties. It is recommended to eat applesauce and also use the fruit in salads. | 200-300 g. |
| You can drink fresh carrot juices. The vegetable is also used in making purees. A small amount of olive oil may be added. | 200-250 g. |
| It can be eaten in its “pure” form, added to salads, and used in the preparation of cold soups. | 200-300 g. |
| — | 150-200 g. |
| It is advisable to eat low-fat products. It is not recommended to add sour cream and sugar. Can be used in preparing light desserts. | 100-150 g. |
| They take a long time to dissolve. You should not chew the candy. | Up to 5 pieces per day. |
| It is advisable to eat classic yoghurts without additives. They can be used in making desserts. | 200-250 g. |
Preventive recommendations
A cyst on the jaw is easily prevented with the help of preventive procedures.
Table 11. Preventive recommendations:
| What to do? | How to do? |
| Teeth should be brushed after every meal and before bedtime. It is advisable to use toothpastes without fluoride. In addition to your teeth, you need to brush your tongue. The use of dental floss and mouth rinses is recommended. The duration of the procedure is 3-4 minutes. |
| Tartar and plaque can only be removed with ultrasonic cleaning. The procedure is performed in a dental office. You should resort to it 1-2 times a year. |
| You should visit the dental office once every six months. This will allow pathology to be detected at an early stage. |
| It is recommended to treat allergies and inflammatory diseases. |
| It is necessary to stop consuming alcohol and tobacco products and minimize the risk of jaw injury. |
All recommendations must be strictly followed. The cost of deviating from them can be very high.
Treatment during pregnancy
If a mandibular cyst forms during pregnancy, the woman should urgently consult a specialist. However, the situation is aggravated by the fact that to confirm the diagnosis it is necessary to take an x-ray. This procedure is dangerous for the fetus. Surgical interventions are indicated only in emergency cases, as they are performed under anesthesia.
When there is no serious inflammation, conservative therapy with medications is carried out. If severe pain and other symptoms are observed, you have to resort to surgery. Therefore, at the slightest discomfort in the oral cavity, you should consult a dentist and gynecologist. You should not use traditional methods, because delaying treatment can lead to severe complications in the lower jaw.
Prevention of the disease There are no specific measures that would completely eliminate the possibility of a jaw cyst. Prevention consists of regular oral hygiene, timely treatment of caries and its complications, as well as all kinds of infectious diseases. Plaque must be removed regularly to prevent it from hardening and turning into tartar.
It is important to visit the dental clinic at least once a year for a preventive examination. This will prevent the development of all kinds of dental diseases. You need to purchase only high-quality brushes and toothpastes, and regularly rinse with special dental elixirs. In case of jaw injuries, you should immediately contact a surgeon and subsequently be observed by him so that complications do not arise.
If you liked the article, please like it.
In the comments, share your experience of treating jaw cysts.