Contracture of the lower jaw: causes, symptoms and treatment features
Mandibular contractures are characterized by reduction of the jaws due to pathological changes in the soft tissues in the facial area. In most cases, this pathology is an acquired disease.
Contracture of the lower jaw: classification and causes
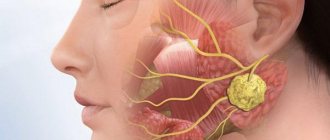
This pathology occurs due to traumatic and inflammatory changes in the joints of the subcutaneous tissue, the skin itself, nerve fibers, masticatory muscles, and parotid-temporal fixation.
Depending on the severity and manifestations of the disease, several types of contractures of the lower jaw are distinguished.
These include temporary (unstable) and persistent pathological processes, as well as congenital and acquired during the patient’s life.
Unstable
Contractures of a temporary nature are expressed in the weakness of the masticatory muscles. Most often they manifest themselves as complications due to prolonged fixation of the jaw (for example, after wearing splints) or as a consequence of the inflammatory process in the tissues of the jaw.
Persistent
Persistent pathologies are caused by deformation of the lower part of the face due to scarring of soft tissues or inflammatory processes. For example, after receiving a gunshot wound to the face, injury to the skull bones, fractures, burns, as well as inflammation of the peri-maxillary tissues.
The appearance of scar contracture of the lower jaw is often associated with diseases such as ulcerative stomatitis, syphilis, and ulcerative necrotizing gingivitis.
Due to changes in soft tissues, limited mobility of the lower part of the face develops, which leads to a significant deterioration in the patient’s quality of life, up to serious deformation of the facial skeleton, especially if scars form in several perimaxillary areas at once.
Contracture of the lower jaw after anesthesia may occur due to violation of the technique of the procedure. In this case, the disease belongs to a number of inflammatory diseases.
There are three degrees of contracture of the lower jaw:
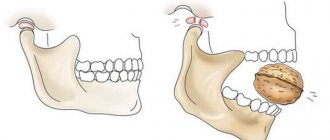
- The first is that the patient’s mouth opening is slightly limited. The distance between the surfaces of the central teeth of the upper and lower jaw is 3-4 cm.
- The second is limiting mouth opening within 1-1.5 cm.
- Third - the mouth opens no more than 1 cm.
Congenital and acquired pathologies
Congenital changes in jaw tissue and skeletal bones are quite rare. Acquired pathologies of a permanent and temporary nature that arise as a result of weakening of the facial masticatory muscles deserve much more attention.
In some patients, the development of contracture of the lower jaw is caused by spasticity (tension) of the muscles against the background of hysterical conditions. In such cases, a person experiences temporary facial paralysis associated with muscle tension in the lower part of the face.
As a result of mandibular contracture, the patient may experience some of the following symptoms:
- speech disorder;
- difficulty chewing food;
- an increase in interdental spaces, especially in the front row (the teeth are arranged in a fan-shaped manner);
- deformation of the jaw bones;
- underdevelopment of the patient’s lower jaw in comparison with the upper;
- noticeable displacement of the lower jaw when opening the mouth.
How are contractures treated?
To eliminate mandibular pathologies, a surgical method is used, aimed at restoring the elasticity of facial tissues, as well as the motor functions of deformed muscles.
The operation is performed under general anesthesia by excision of scar tissue or a longitudinal incision of the scar, followed by its replacement with healthy tissue taken from areas adjacent to the scar or other parts of the patient’s body.
Minor scars can be successfully eliminated using the Limberg method (using triangular flaps).
To treat contracture of the lower jaw caused by the formation of flat scars, complete excision of the scar tissue is performed. The wounds resulting from excision are closed with thin flaps of skin taken from the surface of the patient's body.
In cases where scar removal leads to large-scale losses of soft tissue, leading to exposure of the patient's masticatory muscles, the Filatov method is used to compensate for the lost areas.
This is a plastic method that involves transplanting a rolled-up flap of the patient’s skin, excised along with the subcutaneous tissue (Filatov’s stalk).
This method is often used for deformities caused by deep scar formations in the tissues of the skin, subcutaneous tissue, muscles and mucous membranes of the oral cavity.
In cases of surgical elimination of deformation of the lower jaw caused by the formation of scars in the area of the masticatory muscles, they are cut off from the lower jaw. In the presence of multiple scars formed in the adjacent tissues, in some cases it is impossible to achieve the result of the patient opening the mouth independently.
In such situations, the surgeon inserts a special screw expander. The muscle cut off during the operation grows to the branch of the lower jaw in a new place.
The success of restoring lost muscle functions in the future depends on correctly selected rehabilitation methods and the quality of performance of the therapeutic exercises prescribed by the rehabilitologist.
Inflammatory contracture of the lower jaw is treated by eliminating the source of the infectious process. In the postoperative period, mandatory rehabilitation measures are carried out, including mechanical and physical therapy, as well as therapeutic exercises.
The meaning of gymnastics
In terms of restoring lost jaw functions, primary place is given to physical therapy not only in the early postoperative period, but also in the treatment of contractures caused by injuries and diseases. The final result of the operation performed by the surgeon largely depends on the quality of rehabilitation measures and correctly selected therapeutic exercises to develop the jaw muscles.
You can perform the exercises independently in front of a mirror or in a group of patients suffering from similar disorders, under the guidance and supervision of an instructor.
A set of exercises for recovery
A gymnastics lesson, as a rule, consists of several sequentially performed parts:
- An introductory or preparatory part, consisting of general hygiene exercises performed for about ten minutes.
- The special part of the lesson includes exercises selected individually for each patient in accordance with the clinical picture of the disease. A special set of exercises, depending on the nature of the postoperative period, is introduced already on the eighth day after surgery, in severe cases - on the twelfth day after surgery and at a later date.
- The final stage, like the introductory part, consists of general exercises.
A special set of exercises may consist of movements such as:
- Movements of the lower jaw and head in different directions.
- Facial movements performed to restore the functions of the facial muscles, for example, exercises for the cheeks and lips (puffing out the cheeks, stretching the lips in the shape of a smile or a tube, grinning and other movements).
To consolidate the results obtained, it is recommended not to stop exercising after discharge and postoperative rehabilitation measures. It is necessary to repeat the exercises at home constantly.
Prevention measures
As a rule, the prognosis for the outcome of operations to eliminate the causes of contracture is favorable.
However, to prevent relapses, doctors recommend continuing rehabilitation after discharge from the hospital, in particular, undergoing treatment with special devices for six months after discharge from the hospital (mechanotherapy), performing therapeutic exercises prescribed by the doctor, and undergoing a repeat course of physical therapy.
If all indications are followed, the likelihood of relapses is significantly reduced, and the final result of the operation improves in more than 50% of cases.
Usually the pathological process does not recur, except in cases of incomplete removal of scar tissue.
Most often, young patients undergoing surgery under local anesthesia, which does not allow the cause of the contracture to be completely eliminated, are susceptible to renewed contracture of the lower jaw.
In some cases, children who evade compliance with prescribed rehabilitation measures are susceptible to relapse.
In the treatment of such pathologies in children, it is important to perform the operation efficiently the first time, and then immediately recommend that the patient eat rough food (hard fruits, raw vegetables, crackers, nuts or candies), which helps develop the jaw muscles.
Source: https://FB.ru/article/389566/kontraktura-nijney-chelyusti-prichinyi-simptomyi-i-osobennosti-lecheniya
Treatment of contracture of the lower jaw
The type and nature of treatment measures depend on the location of the scarred tissue and the duration of the disease from the moment the restriction of mouth opening appears until seeking medical help.
In case of ossifying myositis of the masticatory muscle, the ossified portion of the muscle and excess bone tissue along with the periosteum in the region of the lower jaw branch are removed.
In patients with scar changes in the mucous membrane and underlying tissues of the retromolar and posterior sections of the buccal region, the affected tissue is excised until the movements of the lower jaw are restored. The defect is covered with musculocutaneous flaps including the sternocleidomastoid muscle on the upper pedicle. Surgical intervention is recommended to be carried out in two stages: in the first stage, a flap is formed and prepared, in the second stage, contracture is eliminated by excision of scar tissue and closing the defect with a pedicle flap.
For post-injection contractures, mechanical separation of the jaws is effective. Bilateral anesthesia is carried out according to Bershe-Dubov with a 2% lidocaine solution or another anesthetic and jaw redressing. This procedure is accompanied by a clearly audible cracking sound due to the rupture of the cicatricial commissure between the ramus of the mandible and the medial pterygoid muscle. After this, the mouth opens freely. The next day after such a procedure, the volume of mouth opening decreases again, as patients spare themselves due to illness. Anesthesia according to Bershe-Dubov and mechanical opening of the mouth to normal are repeated, which is no longer accompanied by noise phenomena. The implementation of such procedures depends on the period elapsed after the development of contracture (on average 2 weeks) and active mechanotherapy. After the first 3 days, such therapeutic measures are carried out at intervals of 2-3 days and the results are consolidated with physiotherapeutic procedures.
During anesthesia, various complications may occur, which almost always require emergency therapeutic measures.
Contracture of the lower jaw
September 3, 2014
Maksim
Category: TMJ Disorders
12182
Contracture means a sharp limitation of the mobility of the lower jaw due to pathological changes in soft tissues functionally associated with the TMJ (temporomandibular joint).
Impaired movements of the lower jaw and, as a result, impairment of its function can be due to various reasons. There are inflammatory, cicatricial and post-injection contractures of the lower jaw. There are also contractures of the central descent associated with damage to the central structures of the trigeminal nerve (neuroinfections).
In patients who, instead of an anesthetic, are mistakenly injected with irritating substances available in the dentist's office (hydrogen peroxide, ammonia), tissue necrosis and subsequent scarring occur at the injection site.
As a result of violation of the technique of mandibular or torusal anesthesia, damage to nerves or muscles occurs, and the formation of hematomas in the pterygo-maxillary space. The adhesive process in the muscle, between the muscle and the periosteum creates conditions for the development of persistent contracture of the lower jaw.
The causes of the development of cicatricial extra-articular contracture can be trauma, including gunshot, with damage to the masticatory muscle and the subsequent development of myositis ossificans.
Symptoms of contracture of the lower jaw
There is a sharp limitation in mouth opening (up to 1-1.5 cm). During an external examination, an increase in the volume of soft tissue in the area of the projection of the masticatory muscle on one side is sometimes noted (patients with myositis ossificans and inflammatory processes) or the presence of scar tissue in the middle zone of the face or oral cavity.
When palpating the TMJ, no changes in the shape and position of the articular heads of the condylar processes are clinically determined, although the volume of their movements is significantly reduced. Clinically, only minor movements of the heads of the condylar process in the articular fossa are detected.
The volume of lateral movements of the lower jaw to the sides is preserved with some limitation on the side of the contracture. The bite in all patients was not impaired.
Such a symptom as limited mouth opening requires a thorough examination of patients to exclude acute odontogenic inflammatory processes in the cellular spaces (abscess, phlegmon), cancer, damage to the elements of the articulation in the form of fibrous or bone ankylosis and dysfunction of the TMJ with the anterior block of the articular disc.
Differential diagnosis is facilitated by a thorough clinical and x-ray examination of the dental system.
As a rule, X-ray examination of patients in this group does not reveal changes in the bone structures of the lower jaw and TMJ.
Only with myositis ossificans, it is possible to identify various forms of additional intense shadow in the projection of the muscle, and in patients with cancer, changes in the jaw bones.
Treatment of contracture of the lower jaw
The type and nature of treatment measures depend on the location of the scarred tissue and the duration of the disease from the moment the restriction of mouth opening appears until seeking medical help.
In case of ossifying myositis of the masticatory muscle, the ossified portion of the muscle and excess bone tissue along with the periosteum in the region of the lower jaw branch are removed.
In patients with scar changes in the mucous membrane and underlying tissues of the retromolar and posterior sections of the buccal region, the affected tissue is excised until the movements of the lower jaw are restored.
The defect is covered with musculocutaneous flaps including the sternocleidomastoid muscle on the upper pedicle.
Surgical intervention is recommended to be carried out in two stages: in the first stage, a flap is formed and prepared, in the second stage, contracture is eliminated by excision of scar tissue and closing the defect with a pedicle flap.
For post-injection contractures, mechanical separation of the jaws is effective. Bilateral anesthesia is carried out according to Bershe-Dubov with a 2% lidocaine solution or another anesthetic and jaw redressing.
This procedure is accompanied by a clearly audible cracking sound due to the rupture of the cicatricial commissure between the ramus of the mandible and the medial pterygoid muscle. After this, the mouth opens freely. The next day after such a procedure, the volume of mouth opening decreases again, as patients spare themselves due to illness.
Anesthesia according to Bershe-Dubov and mechanical opening of the mouth to normal are repeated, which is no longer accompanied by noise phenomena. The implementation of such procedures depends on the period elapsed after the development of contracture (on average 2 weeks) and active mechanotherapy.
After the first 3 days, such therapeutic measures are carried out at intervals of 2-3 days and the results are consolidated with physiotherapeutic procedures.
Source: https://stom-portal.ru/khirurgiya/zabolevaniya-vnchs/kontraktura-nizhnej-chelyusti.html
Symptoms of contracture of the lower jaw
There is a sharp limitation in mouth opening (up to 1-1.5 cm). During an external examination, an increase in the volume of soft tissue in the area of the projection of the masticatory muscle on one side is sometimes noted (patients with myositis ossificans and inflammatory processes) or the presence of scar tissue in the middle zone of the face or oral cavity. When palpating the TMJ, no changes in the shape and position of the articular heads of the condylar processes are clinically determined, although the volume of their movements is significantly reduced. Clinically, only minor movements of the heads of the condylar process in the articular fossa are detected. The volume of lateral movements of the lower jaw to the sides is preserved with some limitation on the side of the contracture. The bite in all patients was not impaired. Such a symptom as limited mouth opening requires a thorough examination of patients to exclude acute odontogenic inflammatory processes in the cellular spaces (abscess, phlegmon), cancer, damage to the elements of the articulation in the form of fibrous or bone ankylosis and dysfunction of the TMJ with the anterior block of the articular disc.
Differential diagnosis is facilitated by a thorough clinical and x-ray examination of the dental system. As a rule, X-ray examination of patients in this group does not reveal changes in the bone structures of the lower jaw and TMJ. Only with myositis ossificans, it is possible to identify various forms of additional intense shadow in the projection of the muscle, and in patients with cancer, changes in the jaw bones.
Contracture of the jaw after anesthesia. Complications during and after anesthesia in the maxillofacial area
Effective pain relief plays a huge role in the quality of further treatment. Various types of anesthesia are used in dentistry. The choice of method depends on certain indicators. The conduction technique remains the most effective and popular.
After the injection, loss of pain sensitivity occurs over a significant area of the maxillofacial area. This allows you to remove several adjacent teeth, open abscesses and cellulitis, and remove some tumors.
The anesthetic is released near the nerve trunk. This method is called perineural in dentistry. The active substance solution is administered in a smaller volume than with infiltration anesthesia.
Blocking of nerve trunks occurs when bone formations directly exit the natural openings. This results in anesthesia of peripheral receptors. The needle insertion points on the upper jaw are in the area of the natural tubercle, infraorbital, incisive and palatine foramen.
On the lower side, anesthesia is carried out more often at the location of the mandibular and mental foramina.
Indications for use
Blocking the nerves of the lower jaw is performed in the following cases:
- treatment of complicated caries;
- opening of foci of inflammation accompanied by the formation of exudate;
- jaw fractures;
- in the complex treatment of paresthesias, neuritis, neuralgia and contractures;
- orthopedic intervention;
- treatment of periodontal diseases and other soft tissues of the mouth;
- if general anesthesia is not possible;
- when other methods are ineffective.
Rules for local anesthesia
The conduction technique is quite complex. To carry out high-quality manipulation, the dentist must be motivated by certain requirements. This will avoid serious complications and achieve maximum effect. These requirements include the following:
- collect a complete history of the patient’s life and illness;
- choose the right anesthetic;
- clearly know the anatomical structure of the lower jaw;
- the temperature of the anesthetic should be equal to the patient’s body temperature;
- observe the speed of solution administration;
- before inserting the needle, the injection site should be treated and preliminary anesthesia should be performed;
- before the injection, the patient must be explained about the sensations;
- maintain sterility during preparation and manipulation;
- do not leave the patient unattended after the injection;
- Before continuing dental surgery, it is necessary to clarify the effectiveness of anesthesia in the patient.
Mandibular anesthesia
Performed to block the lingual and inferior alveolar nerves. The execution method provides two main methods:
In turn, it is divided into a palpation method, in which a needle is inserted 1 cm above the chewing surface of the 3rd molars of the lower jaw, to the inner surface of the temporal ridge.
The needle is advanced until it makes contact with the bone. As progress progresses, the anesthetic is necessarily released in small quantities. This is necessary to anesthetize the lingual nerve.
After contact, the syringe is moved to the lateral and central incisors, then the needle is advanced another 2 cm.
Another intraoral method is called apodactyl. The landmarks for anesthesia are the pterygomandibular fold. The needle is inserted into its lateral (outer) slope. The injection point is the middle of the intersection of the 2 lines. The first line runs vertically along the outer slope of the fold and the second line runs horizontally between the last chewing teeth in the middle of the fold.
It is a rather complex manipulation. Performed when it is not possible to provide anesthesia in the oral cavity (trismus, fracture). The first access is from the submandibular region.
A needle is inserted at the base of the jaw bone in the middle of the distance of the line running from the upper part of the tragus of the ear to the beginning of the masticatory muscle, retreating 15 mm from the anatomical angle.
Advance the needle parallel to the back of the lower jaw without losing contact with it. In another method, the needle is inserted 2 cm from the base of the tragus anterior to the conditional line.
Move it strictly horizontally to the same distance.
This conduction technique allows you to relieve sensitivity from teeth 1-8, the mucous membrane of the alveolar process, the sublingual area, the lower lip, and part of the skin of the chin. The effect occurs within 10-15 minutes and lasts up to 2 hours. However, the innervation from mid-5 to mid-7 may be completely preserved, since this zone is provided by the sensitivity of the buccal nerve.
Complications after mandibular anesthesia
Unfortunately, after anesthesia, both on the upper and lower jaws, it is sometimes accompanied by some complications. The main problems may be:
Occurs when the rules for injection procedures are not followed. Typically the fracture occurs in the cannula area. Its extraction is carried out in a hospital setting, but according to certain indications. It occurs frequently because, unlike the upper jaw, the needle is inserted very deeply into the soft tissue.
It is observed as an independent phenomenon as a result of anesthetic contact with the trunk of the facial nerve.
- Contracture of the pterygoid muscle.
Basically, there is a violation of the contractility of the internal muscle. In this case, physiotherapeutic procedures and massage are prescribed.