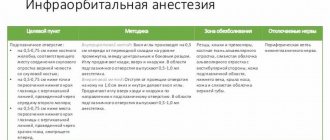
Features of the procedure
Complex anatomical characteristics of the drug administration area increase the risk of complications and reduce the effectiveness of anesthesia. Let's consider some points.
In the temporopterygoid space above the upper jaw there is a venous plexus. It occupies the area from the lower orbital fissure to the lower jaw. Accidental puncture of the venous wall causes the formation of an extensive hematoma, which is quite difficult to prevent.
Inserting the needle at an insufficient level results in the solution being injected into the subcutaneous fatty tissue. In this case, tuberal anesthesia will not be effective at all. Exceeding the depth of needle insertion leads to the following consequences:
- Injection of an anesthetic into the area where the optic nerve is located causes temporary blindness.
- Injecting the drug into the orbital tissue causes temporary strabismus.
- If the solution enters the pterygoid muscle, it causes severe pain after the anesthetic wears off.
The tip should not be allowed to slide along the tubercle during the procedure, as it may perforate nerves and small vessels.
Pain relief zone
Tuberal anesthesia in dentistry allows you to anesthetize the following areas:
- area of the upper molars;
- the periosteum and the mucous membrane of the alveolar process covering it;
- mucosa and bone of the maxillary sinus along the posterior wall.
The border area of anesthesia passing behind is constant. In front, it can reach the middle of the first small molar and, accordingly, the mucous membrane located in this area along the gum.
Intraoral tuberal anesthesia according to Egorov
Progress of the procedure:
- The patient's mouth is half open. Hold the cheek with a spatula.
- Directing the bevel of the needle towards the bone tissue, the doctor makes a puncture at the level of the second molar to the bone.
- The needle should be positioned at an angle of 45° to the alveolar process.
- The needle moves up, back and towards the middle, while it is necessary to control its constant contact with the bone. A small amount of anesthetic is released along the way.
- The needle is inserted 2-2.5 cm. The piston is pulled back to check that the vessel has not been punctured.
- If there is no blood, up to 2 ml of solution is injected. The syringe is removed.
- The patient presses the anesthesia site to avoid the formation of a hematoma.
- The full effect of the drug appears within 10 minutes.
If you use a short-acting anesthetic, the procedure will be effective for 45 minutes, if long-acting - up to 2.5 hours. Intraoral tuberal anesthesia is performed for outpatient operations and for simultaneous intervention on several molars.
Methods of pain relief on the lower jaw
1. Subzygomatic method of anesthesia of the second and third branches of the trigeminal nerve
(according to Weisblatt).
The feasibility of this method is determined by the relative ease and safety of its implementation.
With this method, the needle is inserted directly under the lower edge of the zygomatic arch and advanced through the notch of the mandibular ramus towards the base of the outer plate of the pterygoid process.
The guideline for the correct direction of the needle with this method is the outer plate of the pterygoid process.
Its projection onto the skin is located midway from the base of the tragus of the auricle to the outer corner of the eye.
| Rice. Anesthesia according to Weisblatt |
Injection technique.
After treating the patient’s facial skin with alcohol, use a sterile ruler under the zygomatic arch to measure the distance from the tragus of the auricle to the outer edge of the eye and mark the middle of this distance on the skin. A sterile rubber circle with a diameter of about 5 mm is threaded onto a 6 cm long needle and the needle is placed on a 10 gram syringe.
At the marked point, a needle is inserted and, using an anesthetic solution, it is advanced perpendicular to the surface of the skin until it stops at the outer plate of the pterygoid process. Having marked the depth of immersion of the needle with a rubber circle, it is brought out approximately half of the marked distance. To anesthetize the second branch of the trigeminal nerve, the needle is directed anteriorly at an angle of 20-25°, without changing its position in the horizontal plane. Having moved it deeper to the length marked with a rubber circle, they reach by entering the pterygopalatine fossa, where 3-120 ml of anesthetic is released.
The anesthesia zone extends to the corresponding half of the upper and lower jaw.
2. Anesthesia of the third branch of the trigeminal nerve according to V.M. Uvarov.
V. M. Uvarov proposed injecting a needle under the zygomatic arch 2 cm anterior to the tragus of the ear, advancing the needle deep into the soft tissues so that it passed through the notch of the mandibular ramus immediately in front of the condylar process, and plunging it 4-4 deep .5 cm, reach the foramen ovale, where 5-6 ml of anesthetic is injected.
3. Anesthesia of the inferior alveolar nerve in the area of the mandibular opening
(mandibular anesthesia).
This method is called mandibular, although the mandibular nerve is not blocked. At the opening of the lower jaw, its branches are blocked - the lower alveolar and lingual nerves. To properly administer anesthesia, it is necessary to know the anatomy of the lower jaw, especially its branches.
| Rice. a — the position of the end of the needle in relation to the vascular bundle of the lower jaw during conduction anesthesia; b — landmarks of the needle insertion site for mandibular anesthesia |
The inferior alveolar nerve enters the bony canal through the foramen of the mandible.
It is located on the inner surface of the mandibular ramus at a distance of 15 mm from the anterior edge, 13 mm from the posterior edge, 22 mm from the mandibular notch and 27 mm from its base. In an adult, the opening of the lower jaw is located at the level of the chewing surface of the lower molars. For old people and children it is slightly lower. It is covered from the front and from the inside by the tongue of the lower jaw, so the anesthetic should be injected 0.75-1 cm above that opening, before the nerve enters the canal.
Intraoral methods
- Anesthesia by palpation of bony landmarks.
The reference point for inserting the needle is the temporal ridge, which in the form of a bone ridge descends from the coronoid process to the lingual surface of the alveolar process of the mandible. In the lower section it is divided into two legs, which form a triangle. The anterior edge of the mandibular ramus is palpated with a finger at the level of the posterior surface of the crown of the third molar. The temporal ridge is identified by moving the finger slightly inward, and its projection is transferred to the mucous membrane. Then the finger is fixed in the retromolar fossa.The needle is inserted medially from the projection of the temporal ridge and 0.75-1 cm above the chewing surface of the third molar, placing the syringe at the level of the premolars of the opposite side. Having advanced the needle outward and backward to the bone by 0.5-0.75 cm, 0.5-3 ml of anesthetic is injected, the lingual nerve is turned off, advancing the needle another 2 cm, they reach the point where the inferior alveolar nerve enters the canal. Here 2-3 ml of anesthetic is injected. Without changing the initial position of the syringe, it is not always possible to advance the needle to the opening of the lower jaw. This can be achieved by moving the syringe to the level of the central incisors and moving the needle posteriorly 2 cm parallel to the inner surface of the mandibular ramus.
- Apodactyl method.
The reference point is the pterygomandibular fold, which is located medially from the temporal crest.The patient's mouth is wide open. The syringe is placed at the level of the premolars of the opposite side. The injection is made into the outer edge of the pterygomandibular fold in the middle of the distance between the chewing surfaces of the upper and lower molars. If the fold is wide, then the needle is inserted into the middle; if it is narrow, then into its medial edge. The needle is advanced outward and posteriorly to the bone (to a depth of 1.3-2 cm). 2-3 ml of anesthetic is injected, turning off the inferior alveolar and lingual nerves. Sometimes a needle immersed 2 cm into soft tissue does not touch the bone. In this case, the syringe must be retracted even more in the opposite direction, placing it at the level of the second molar.
Extraoral methods
- From the submandibular region.
A needle is inserted at the base of the lower jaw, 1.5 cm anterior to its angle. The needle is advanced 3.5 cm upward along the inner surface of the mandibular ramus strictly parallel to its posterior edge. Be sure to maintain needle contact with the bone. It is more convenient to insert the needle without a syringe and attach it only before administering the anesthetic. 2 ml of anesthetic is injected to block the inferior alveolar nerve. By moving the needle up another 1 cm, the lingual is blocked.Rice. Extraoral method of anesthesia of the inferior alveolar nerve - Subzygomatic method according to Bershe-Dubov.
Place the needle perpendicular to the skin of the lateral surface of the face. The needle is inserted directly under the lower edge of the zygomatic arch, 2 cm anterior to the base of the ear tragus. The needle is advanced 3-3.5 cm inward, introducing an anesthetic. 3-5 ml of anesthetic is injected.
Anesthesia zone for mandibular anesthesia
.
All teeth of the lower jaw of the corresponding half, bone tissue of the alveolar part and partly of the lower jaw, mucous membrane of the alveolar process on the oral and vestibular side, mucous membrane of the sublingual region and anterior 2/3 of the tongue, skin and mucous membrane of the lower lip, skin of the chin on the side of anesthesia.
Pain relief occurs within 7-15 minutes. The duration depends on the anesthetic chosen.
| Rice. Anesthesia zone for: a - mandibular anesthesia; b — torusal anesthesia |
4. Thorusal anesthesia according to Weisbrem
.
An anesthetic solution is injected into the area of the mandibular ridge, where the inferior alveolar, lingual and buccal nerves, surrounded by tissue, are located.
The patient's mouth should be as open as possible. The injection site is the point formed by the intersection of a horizontal line drawn 0.5 cm below the chewing surface of the upper third molar and the groove formed by the lateral slope of the pterygomandibular fold of the cheek. The needle is inserted strictly perpendicular to the tissues of the cheek, directing the syringe from the opposite side, it is advanced to the bone to a depth of 0.25-2 cm.
1.5-2 ml of anesthetic is injected, turning off the lower alveolar and buccal nerves, then, withdrawing the needle in the opposite direction, 0.5-1 ml of anesthetic is injected to turn off the lingual nerve. Anesthesia occurs within 5 minutes.
| Rice. Thorusal anesthesia |
Anesthesia zone: the same tissues as during anesthesia at the opening of the lower jaw, as well as the mucous membrane of the cheek and skin, the mucous membrane of the alveolar part of the lower jaw from the middle of the second premolar to the middle of the second molar.
5. Anesthesia at the mental foramen (mental).
The mental foramen is located 12-13 mm above the base of the body of the lower jaw, at the level of the middle of the alveolus of the lower second premolar or the interalveolar septum between the first and second premolars. The mental foramen opens posteriorly, upward and outward.
Extraoral method.
If anesthesia is performed on the right half of the lower jaw, the doctor should stand to the right and behind the patient. The needle is inserted 0.5 cm above and behind this point, giving the needle a direction taking into account the course of the canal, inward and anteriorly until it contacts the bone. 0.5 ml of anesthetic is injected. Carefully use a needle to find the entrance to the canal and insert the needle to a depth of 3-5 mm. 1-2 ml of anesthetic is administered, pain relief occurs after 5 minutes.
| Rice. Needle position for submental anesthesia |
Intraoral method.
The patient's teeth should be closed. The cheek is retracted and the injection is made at the level of the middle of the crown of the first molar, retreating a few millimeters outward from the lower arch of the vestibule of the mouth. The needle is advanced to a depth of 0.75-1 cm downwards, anteriorly and inward to the mental foramen. The remaining aspects of anesthesia are the same as with the extraoral method.
Pain relief zone:
soft tissues of the chin and lower lip, premolars, canines and incisors, bone tissue of the alveolar part, mucous membrane of the vestibular side. Sometimes the zone of anesthesia extends to the level of the second molar.
6. Berche anesthesia to eliminate inflammatory contracture.
This anesthesia anesthetizes the motor fibers of the third branch of the trigeminal nerve. The needle is injected perpendicular to the skin under the zygomatic arch 2 cm anterior to the tragus of the ear and, moving the needle through the semilunar notch of the mandible to a depth of 2-2.5 cm, 3-4 ml of anesthetic is injected. Anesthesia occurs within 10 minutes.
M.D. Dubov modified Berche's method.
When the needle is advanced 3-3.5 cm deep and an anesthetic is introduced here, the latter penetrates the inner surface of the lateral pterygoid muscle and turns off the inferior alveolar and lingual nerves, which are located next to this muscle.
| Rice. Anesthesia according to Bershe-Dubov |
“Practical guide to surgical dentistry” by A.V. Vyazmitina
Published by Konstantin Mokanov
Extraoral method
Regardless of which side tuberal anesthesia is needed, the technique requires tilting the patient's head in the opposite direction. Before the anesthesia itself, the doctor determines the depth to which the needle will need to be inserted. This is the distance between the lower outer corner of the orbit and the anterior lower corner of the zygomatic bone.
The dentist is positioned to the patient's right. The needle is inserted in the area of the anteroinferior angle of the zygomatic bone. It should have an angle of 45° with respect to the midsagittal plane and a right angle to the trago-orbital line. After inserting the needle to the desired depth, an anesthetic is injected. Pain relief develops over 5 minutes.
Technique of conduction anesthesia in dentistry
The principle of the technology is that the medicine is injected into the area where the nerve is located, which will eventually block pain symptoms in the entire desired area. The medicine gets into the desired area through a puncture. As we mentioned, it is very important to correctly calculate the distance at which the needle is inserted. To do this, doctors use either ultrasound, the technology of which is basically known to everyone these days, or a neurostimulator, which is used to determine the distance from the nerve to the needle.
The puncture itself is a painless procedure, the patient will feel only minor discomfort. When the medicine is administered, a “tissue swelling” effect is possible, which will pass very quickly. The effect of the anesthetic occurs quite quickly; almost immediately after the injection, the lower lip of the person who is in the dentist’s chair at that moment will begin to go numb. This is a sure sign that the medicine has worked and you can proceed with the scheduled operation.
In order to determine whether the needle has entered a blood vessel (this can cause hematomas), the doctor slightly pulls the syringe plunger in the opposite direction and looks to see if blood appears. If this happens, the needle is moved, the test is performed again, and, if the result is positive, the medicine is administered.
You can see how a specialist performs conduction anesthesia in dentistry in this video in Russian.
Drugs
Tuberal anesthesia is performed using local anesthetics:
- Lidocaine is the first amide derivative, on the basis of which Bupivacaine, Articaine, Mezocaine and other drugs were synthesized. It is used in the form of a 1-2% solution. Lidocaine belongs to drugs in the low price category. Contraindicated in patients with organic liver damage.
- Trimecaine is an amide derivative. In terms of its effectiveness, speed and duration of action, it is several times superior to Novocaine. Available in the form of solutions of various concentrations. As a side effect of the administration of the drug, pale skin, nausea, and headache may occur.
- The drug "Ultracain", the price of which is 1.5-2 times higher than that of other representatives of local anesthetics (50 rubles per ampoule), has a greater advantage in use. High diffusion ability and good duration of action allow it to be used not only in surgical, but also in orthopedic dentistry. How much does Ultracaine cost? The price of the drug (for anesthesia with this particular drug in Russian dental clinics you will have to pay from 250 to 300 rubles) is explained by its foreign origin. Analogs - “Artikain”, “Alfacain”, “Ubistezin”.
All products are used in combination with a vasoconstrictor (adrenaline). When choosing a drug, the specialist determines individual tolerance and the maximum dose, takes into account the patient’s age, as well as the presence of pregnancy and concomitant pathologies.
Complications of the procedure
Tuberal anesthesia, reviews of which are mixed (patients note an excellent analgesic effect, but some complain that the numbness does not go away for a long time, up to 5 hours, plus the side effects already mentioned above are not to the liking of many), should be carried out by a highly qualified specialist, able to take into account all the necessary nuances of the event. Some of the possible complications have already been discussed. Time should be devoted to the issue of their prevention.
Injury to blood vessels and the formation of hematomas in the area of anesthesia can be prevented. For this purpose, during anesthesia, you must not lose contact of the needle with the bone tissue and insert it no more than 2.5 cm. After removing the needle, the infiltrate formed by the injected anesthetic is massaged upward behind the maxillary tubercle. Tuberal anesthesia is allowed only in the absence of inflammatory processes at the site of drug administration.
It becomes dangerous for the patient if the solution enters the bloodstream. Its toxicity increases by 10 times, and the effect of a vasoconstrictor - by 40. The patient may experience shock, collapse, or fainting. To prevent such a complication, before injecting the anesthetic, the syringe plunger is pulled back. This makes sure that the needle does not enter the vessel. If blood appears in the syringe, you need to change the direction of the needle and only then inject the drug.
Violation of aseptic rules during the procedure can lead to infection. When inserting a needle into your mouth, you need to be careful that it does not touch the tooth. Plaque exposure will lead to the development of phlegmon.
Conduction anesthesia in dentistry: indications and contraindications
Indications
- Removal of “difficult” teeth, such as chewing teeth
- Removing several teeth at once
- Removal of various types of formations in the mouth
- Opening purulent abscesses
- Maxillofacial surgeries
Contraindications
- First of all, this is, of course, an allergy to the injected medicine
- Those surgical interventions for which another type of anesthesia will be more effective
- Cardiovascular diseases
- Diabetes
- Lack of contact with the patient: deafness and mental illness
- Pregnancy
- Due to its specificity, this type of anesthesia is not used if, for one reason or another, the patient has experienced topographic changes in the jaw area