Purpose of the dental system
The biological mechanics of the dental system and its understanding lead to timely recognition of pathologies of teeth and soft tissues of the oral cavity. The normal functioning of the temporomandibular joint largely depends on the structure and normal functioning of the periodontium - the soft tissues surrounding the tooth cavity.
The anatomy and physiology of the structure of the periodontium determines the biomechanics of the structure and the characteristics of the periodontium. In addition, periodontal biomechanics helps in the functioning of other organs.
Knowledge of the laws of biological mechanics of the jaw and joints helps to design and use features, as fundamental knowledge on the topic of prosthetics and dental implants. Knowledge of the anatomical features of the jaw is necessary in the manufacture of structures and dental materials.
Devices have been developed that almost completely repeat the movements of the jaw and make it possible to reproduce anatomically similar structures to the human jaw. Popular devices include the occluder, facebow, and articulator. The latter design plays an important role in the fitting and creation of individual prostheses.
If disorders of the lower jaw occur, disruptions in articulation, speech, nutrition and swallowing occur. Today, a system of articulation of movements has been developed, led by such authors as Ganau, Gisi, Monson. These authors most accurately described the biomechanics of mandibular movements.
The authors claim that dysfunction of the lower jaw, as well as sore neck muscles, necessarily lead to breathing problems. Different angles of inclination of the lower jaw determine human health.
Occlusion is a condition characterized by full contact of both jaws, which ensures complete chewing of food. Therefore, the contact of teeth is a determining factor for the characteristics of chewing mechanisms.
The work and action of the lower dentition during chewing is due to the synchronous work of all muscles and joints. The work occurs under the influence of the central nervous system. In this case, displacements that occur spontaneously occur under the influence of the neuromuscular structure.
Conscious movements of the dentition include the moment food enters the mouth and swallowing food. The remaining movements that occur after eating food are the result of unconscious motor functions of the body.
The lower part of the human masticatory apparatus is the only moving bone in the human body. However, the connecting and muscle tissue, which sets the mechanism in motion, is of great importance in the structure of the masticatory row and in the normal functioning of the muscles.
In the structure of the lower dentition, there are several muscle groups that are responsible for various movements of the jaw.
Movements of the lower jaw, bite and occlusal contacts of teeth
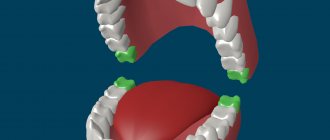
Opening the mouth. The initial position of the lower jaw when opening the mouth is the state when the lips are closed. At the same time, there is a gap of 2-4 mm between the dentition of the lower and upper jaw. This state is called a state of physiological rest.
The lowering of the lower jaw is carried out under the weight of the bone itself and bilateral contraction of muscles: the jaw - the hyoid muscle, the chin - the hyoid muscle, the anterior belly of the digastric muscle. There are 3 phases in the lowering of the lower jaw - slight, significant and maximum lowering. This corresponds to 3 types of movement of the articular heads.
A slight lowering of the lower jaw (quiet speech, drinking) occurs when its head moves in relation to the disc in the “lower floor” of the temporomandibular joint. In this case, identical movements simultaneously occur in the right and left joints along axes running along the greatest length of the ellipsoidal head of the lower jaw, and the midpoint of the central lower incisors describes an arc about 20 mm long.
With a significant lowering of the lower jaw (loud speech, biting) and hinge rotation in the “lower floor” of the joint, the articular heads, together with the discs, slide forward along the circumference of the articular surface, i.e. movement also occurs in the “upper floor” of the joint.
With the maximum lowering of the lower jaw, the sliding of the heads is delayed at the top of the articular tubercle by the tension of the articular capsules, articular ligaments and muscles. In this case, the midpoint of the lower incisors describes an arc up to 50 mm long.
Further excessive opening of the mouth can also occur with a slight hinge movement of the articular heads, but this is highly undesirable, since there is a danger of stretching of the ligamentous apparatus of the temporomandibular joint, dislocation of the head and disc.
Closing the mouth. Raising the lower jaw is carried out by contracting the muscles that lift the lower jaw (masseter, temporal, medial pterygoid) and the movements occur in the reverse order. The articular heads are displaced back and upward to the base of the slopes of the articular tubercles. The closing of the mouth is completed due to the hinge movements of the articular heads until occlusal contacts appear.
Movement of the lower jaw forward. After reaching the initial contact of the chewing teeth (centric relation), the articular heads move forward and upward - into central occlusion. At the same time, they move 1-2 mm along the midsagittal plane, without lateral displacements, with simultaneous bilateral contact of the slopes of the cusps of the lateral teeth.
The advancement of the lower jaw forward with the teeth closed from the central occlusion to the anterior one is carried out due to the contraction of the external pterygoid muscles on both sides. This movement is guided by the incisors. If the lower incisors in central occlusion are in contact with the palatal surfaces of the upper incisors, moving the lower jaw forward from this position causes disocclusion of the lateral teeth. The sliding continues until the cutting edges of the teeth of the lower jaw come into contact with the cutting edges of the teeth of the upper jaw. The path that the lower incisors take along the palatal surfaces of the upper incisors is the sagittal incisal path, and the angle between this path and the occlusal plane is the angle of the sagittal incisal path. During this movement, the articular heads move forward and down the slopes of the articular tubercles, making a sagittal articular path, and the angle between this path and the occlusal plane is called the angle of the sagittal articular path.
These angles and their individual determination for each patient are used to adjust the articulator - a device that simulates the movement of the lower jaw.
When moving the lower jaw forward between the dentition, contact is maintained at several points: between the incisors, between individual chewing teeth on the left and right sides. The cusps of the last molars of the lower jaw stand above the level of the cusps of other chewing cusps of the first and second molars of the upper jaw below the level of its other chewing teeth. These contacts in the literature are called the three-point Bonville contact or the Bonville triangle point. The sides of the triangle connect the centers of the right and left articular processes of the lower jaw and the incisal point and average 10 cm.
Lack of contact in the area of chewing teeth when biting, when there is occlusal contact on the incisors, can lead to overload of the latter, and with artificial dentition replacing a defect in the front teeth or a complete defect in the dentition (dentitions) - to the overturning of the dentures. This can cause overload of the joint, since the intra-articular disc, moved to the top of the articular tubercle, experiences increased pressure from the articular head, and the capsule and ligaments of the joint are stretched. If a three-point contact (according to Bonneville) is created on artificial dentition, then the pressure on the joint discs is reduced, the ligaments are stretched less, and the fixation of the prosthesis is better.
Lateral movements of the lower jaw
Rice. 10. Scheme of lateral movement of the lower jaw to the left in the horizontal plane (a), possible paths of movement of the head of the balancing side (b) and the “occlusal compass” (c):
A, B - initial position of the jaw;
A1, B1 - position of the jaw when shifted to the left;
B – B1 – Bennett movement;
B is Bennett's angle. The dotted line indicates “initial lateral movement”;
c - “occlusal compass” - a path that describes the supporting palatal cusp of the upper left first molar on the occlusal surface of the lower first molar shown in the figure;
E – forward movement;
G – movement to the left;
D – movement to the right.
During lateral movement of the mandible from the position of central occlusion, the articular head on the side of displacement (side of laterotrusion) rotates around its vertical axis in the corresponding glenoid fossa and makes a lateral movement, which is called Bennett's movement. This lateral movement of the working articular head averages 1 mm. The articular head on the opposite side (the mediotrusion side) moves downwards, forwards and inwards. The angle between this path of head movement and the sagittal plane is Bennett's angle (~ 17º). The greater the Bennett angle, the greater the amplitude of the lateral displacement of the articular head of the balancing side.
With a lateral displacement of the lower jaw, the lateral pterygoid muscle of the side opposite to the displacement of the lower jaw contracts, therefore, with a unilateral type of chewing, unilateral hyperactivity of the muscle can occur, which adversely affects the function and structure of the TMJ, the condition of the hard tissues of the teeth and periodontium.
When studying the structure of the dentition of the lower and upper jaws in the area of chewing teeth, the following was established:
a) the crowns of the chewing teeth of the lower jaw are inclined towards the tongue, resulting in an equal level of location of the buccal and lingual cusps;
b) the palatal cusps of the maxillary molars are located lower than the buccal ones.
As a result of different levels of arrangement of the cusps of the chewing teeth, lateral occlusal curves are formed that pass through the buccal and lingual cusps of both sides of the chewing teeth. Lateral occlusal curves ensure the preservation of occlusal contact in the area of the chewing teeth with a lateral shift of the lower jaw, which is equal to no more than half the width of the chewing teeth.
During lateral movements of the lower jaw, the occlusal relationship between the cusps of the antagonist teeth on the balancing and working sides is different. On the side of the contractile muscles, the antagonists meet with tubercles of the same name (working side), on the opposite side - with opposite tubercles (balancing side).
Literature:
- S. I. Abakarov, ed. E. S. Kalivradzhiyan “Fundamentals of dental prosthetics technology - a textbook for medical schools and colleges. Moscow, 2020. M.: “Geotar – Media”. pp. 130 – 146.
- I.V. Alabin, V.P. Mitrofanenko “Anatomy, physiology and biomechanics of the dental system” - M., “ANMI”, 1998, p. 73-93, 99-114, 178-181.
- Shcherbakov A.S., Gavrilov E.N., Zhulev E.N. “Orthopedic dentistry”, St. Petersburg: IKF “Foliant”, 1998, p. 44-51
Original work:
Movements of the lower jaw, bite and occlusal contacts of teeth
Directions of movement of the lower jaw
During the movement of the lower jaw, sagittal, vertical and transversal displacement of its heads occurs.
Vertical displacement is necessary to open and close the mouth. In this case, the movement, depending on the force, occurs with varying strength, which determines the degree of movement of the head.
The sagittal axis of displacement is the ability to move the lower jaw back and forth. In this case, the forward movement of the jaw and the biomechanism of the head of the articular part at the moment of movement is called the sagittal path of the joints.
Transverse is the ability of the jaw to move left or right. In this case, certain muscle groups move. For example, the direction of the masticatory apparatus to the right determines the left direction of the lateral muscles, and vice versa.
Without knowledge of how muscles and joints work, the dentist cannot regulate the normal functioning of the masticatory apparatus, which means he will not be able to manufacture and install suitable dentures and implants.
Dislocation of the lower jaw
First aid consists of reversing the dislocation of the lower jaw under infiltration or conduction anesthesia. To reduce the anterior dislocation of the lower jaw, the methods of Hippocrates, Khodorovich, Blechman, Gershuni, Popescu (for old dislocations) are used. The classic way to reduce bilateral dislocation of the lower jaw is the Hippocratic method: the patient sits on a low chair, so that the back of the head is supported, and the lower jaw is located at the level of the elbow joints of the dentist or traumatologist/surgeon. Standing opposite the patient's face, the doctor places his thumbs, wrapped in a towel or a thick layer of gauze, on the lower molars, and with the rest covers the lower jaw from the outside. Gently pressing down with his thumbs, the doctor moves the jaw back with a small push, quickly removing his fingers from the teeth to avoid biting. The movement of the articular heads of the lower jaw into place is accompanied by a characteristic click and intense closure of the jaws.
When reducing a posterior dislocation after the lower jaw has been displaced downward, it is moved anteriorly. In order to avoid recurrent dislocation of the lower jaw and limit movement in the TMJ after the reduction procedure, it is necessary to immobilize the jaw using a chin sling for 7-10 days (for anterior dislocation) and for 2-3 weeks (for posterior dislocation). Until recovery, the patient is advised to stop eating solid food and follow a gentle diet. If it is impossible to reduce the dislocation of the lower jaw using conservative methods, they resort to the surgical method. For chronic dislocations of the lower jaw, resection of the articular heads of the lower jaw may be required, followed by mechanotherapy.
Patients often learn to adjust habitual dislocations of the lower jaw on their own. Further treatment should include therapy for the underlying disease, wearing it for 2-3 months. medical orthopedic devices and splints that limit mobility in the joint (Petrosov apparatus, Burgonskaya-Khodorovich apparatus, Yadrova splint). According to indications, it is necessary to carry out selective grinding of teeth, prosthetics of missing teeth, blockade of masticatory muscles, massage, therapeutic exercises, physiotherapy (electrophoresis of medicinal substances, galvanization).
Surgical treatment of habitual dislocation of the lower jaw can be aimed at strengthening the ligaments, deepening the articular cavity, increasing the height of the articular tubercle, repositioning and fixing the intra-articular disc.
TMJ functioning problems
| Click to sign up for a FREE consultation |
Disruption of the work and function of the joints and muscles of the lower jaw is called TMJ dysfunction. The pathology is caused by the occurrence of a defect in the teeth, increased wear and tear and an abnormal bite of a person.
The main clinical manifestation of dysfunction is clicking and clattering of teeth when opening the mouth. In more advanced cases, pain occurs in the ears, jaw, and painful sensations begin during chewing and yawning.
The main method for diagnosing TMJ dysfunction is radiography, which reveals dysfunction of the jaw and joint.
Treatment consists of a comprehensive effect on the condition of the jaw, which the dentist carries out based on knowledge of the biomechanics of its work.
Purpose, structure and functioning of the dental system
Understanding the complex process, which is called the biomechanics of the masticatory apparatus of the dentofacial system, contributes to the timely detection of pathology in the development of muscles, articular structures, closure of teeth and the condition of the periodontium (tooth - Greek odontos, Latin dente - hence the formation: odontology - the science that deals with the description of odontos , periodontitis is a disease of periodontal tissues).
It is on a healthy periodontium - the complex of tissues surrounding the tooth, which is a single component of the temporomandibular joints - that its normal functioning depends. It follows from this that the biomechanical functions of the periodontium are determined by the anatomical and physiological features of its structure and are closely related to the work of other elements.
The laws of biomechanics of the dental system are successfully applied in orthopedics at the stages of design and creation of various prostheses, as well as some auxiliary devices.
Devices that reproduce the movements of the lower jaw include:
- Occluder . A device for assisting the patient, allowing to simulate and make the correct adjustment of the orthopedic structure.
- Facial bow . This device allows you to make an impression as accurately as possible for further correction of the bite.
- Articulator . They come in different types: universal, medium (simplified). This device is used for the manufacture and fitting of removable and fixed dentures and bridges, crowns and caps.
Photo:
Occluder
Facebow
Articulator
It is worth noting that the articulator is an extremely important device that helps to correctly make an exclusive fit of various prostheses. After all, it is articulation, in dentistry perceived as a multi-vector movement of the lower jaw (lat. mandibula) relative to the upper one, which occurs during compression and stretching of the masticatory muscles, which decisively determines intelligible and articulate pronunciation.
If some pathology associated with low frequency develops, then speech, chewing food, laughter, and swallowing are immediately impaired.
The table of movements of the lower jaw in a concise form sets out the basic provisions and determining factors of the dominant theories of articulation, the authors of which are Hanau, Gysi, Monson. Despite some discrepancies in the interpretation of the processes, their authority is indisputable, and their role in the development of orthopedics is beyond doubt.
| Articulatory theories of dentition construction | Basic provisions | Determining factors |
| Gysi's theory | The inclination of the articular path determines the displacement vector of the mandibula, which is influenced by the size and shape of the articular tubercle | Accurate determination of the articular path. Recording the incisal path. Determination of the sagittal compensation curve. Determination of the transversal compensation curve of the line. |
| Monson's theory | Complex vector movements of the LF are determined not by the articular paths, but by the surfaces of the dental cusps, which give direction to the movements | |
| Hanau's theory | The theory is similar to Gysi's theory, which analyzes the entire system of articulation. In particular, she highlights the differences between the position of the prosthesis in the articulator and in the mouth due to a decrease in the elasticity of muscle tissue | Inclination of the articular path Depth of the compensation curve Inclination of the reference plane Inclination of the upper incisors Cusp height |
| Balancing theory | Takes into account:
| |
| Spherical theory | Provides:
|
In addition, correct and healthy breathing and aesthetic emotions (expression) are impossible if the muscles that push the lower jaw forward are subject to obstruction (spasm, remission).
Complete chewing of food occurs only if the teeth of the upper and lower jaws come into correct contact - occlusion. Therefore, it is the closure of the dentition that is the defining characteristic of chewing movements.
All connecting elements of the LF move as a result of the synchronous interdependent action of the temporomandibular joint (TMJ), muscular chewing tissues and teeth. Their actions are organized, coordinated and controlled by the central nervous system.
Displacements of a spontaneous and reflex nature are entirely subordinate to the neuromuscular system and can be reproduced consistently.
The initial voluntary movements include the process of biting food and directing it into the mouth. And the following chewing and swallowing are reflexive-unconscious actions.
Due to the tasks that are defined for the jaw, its complex structure is determined.
First of all, it is the only movable bone of the facial skull, which vaguely resembles a horseshoe.
This structure is due not only to its defining purpose as a responsible component of the chewing process, but also to its development, which originates from the first gill arch.
Mandible structure:
- Body.
- The edge of the body where the cells for teeth (alveoli) are located is the alveolar process.
- Chin hole. It serves as a communicator for nerves and blood vessels.
- Corner.
- Head.
- Mandibular canal and foramen.
- Branches.
- Articular and coronoid processes.
The bone formations would remain constantly in a static position if it were not for the muscle tissue connecting them.
The muscles that move the lower jaw are called mastication.
Moreover, each muscle structure, or rather their groups, produces certain movements:
- The medial pterygoid, masseter and temporal muscles raise the jaw.
- The digastric, mylohyoid, and geniohyoid are involved in the process of descent.
- Lateral movements are possible thanks to the lateral pterygoid muscles.
Muscles that lift the mandible (posterior group)
The chewing muscle (m. masseter) starts from the lower edge and inner surface of the zygomatic arch, the anterior slope of the articular tubercle of the temporal bone, and the temporal fascia. It is attached to the masticatory tuberous outer surface of the ramus of the mandible below its notch. From the lower jaw, muscle bundles are directed upward, anteriorly and outward. The masticatory muscle lifts the lower jaw, its superficial layer pushes the jaw forward, and with unilateral contraction, it shifts it in the direction of contraction. The temporal muscle (m.temporalis) has a fan-shaped shape and consists of 3 layers: superficial, middle and deep. It starts from the inner layer of the temporal fascia in the region of the temporal line, the temporal bone, the temporal surface of the greater wing and the infratemporal crest of the sphenoid bone, the parietal, the squama of the frontal, and the temporal surface of the zygomatic bone. Attached to the apex and outer surface of the coronoid process, the branch of the mandible in the area of its notch and the oblique line, the inner surface of the branch of the mandible. From the lower jaw, muscle bundles are directed upward, outward and somewhat backward. The anterior and middle fascicles lift the lower jaw, the posterior fascicles pull the jaw pushed forward backward. The medial pterygoid muscle (m.pterygoideus medialis) has a quadrangular shape. It starts from the walls of the pterygoid fossa of the pterygoid process of the sphenoid bone, the outer surface of the pyramidal process of the palatine bone. Attaches to the pterygoid tuberosity on the inner surface of the angle of the lower jaw (symmetrically with the masticatory muscle). From the lower jaw, muscle bundles are directed upward, inward and anteriorly at an angle of 37-48°. With a bilateral contraction, the muscle lifts the lower jaw and pushes it forward; with a unilateral contraction, the muscle moves the lower jaw to the opposite side and upward. The lateral pterygoid muscle (m.pterygoideus lateralis) has a triangular shape and lies in the infratemporal fossa. It starts with two heads (upper and lower). The superior head originates from the infratemporal surface and infratemporal crest of the greater wing of the sphenoid bone and from the tendon of the deep layer of the temporal muscle. The lower head extends from the outer surface of the pterygoid process of the sphenoid bone. The superior head is attached to the articular capsule and articular disc of the temporomandibular joint; the lower head - to the pterygoid fossa of the condylar process of the mandible. From the lower jaw, the muscle fibers are directed forward and inward. With bilateral contraction, the muscle pushes the lower jaw forward, with unilateral contraction, it moves it to the opposite side [Mikhailov S.S., 1973].
The main muscles involved in the movements of the lower jaw.
Lesson No. 5.
The structure and functions of the temporomandibular joint, the main muscles that carry out movements of the lower jaw in various directions, their functions. The structure of the dentition. Occlusion and articulation. Types of occlusion. Bite. Types of bite. Occlusiometry.
Required: film “biomechanics”, occluder with teeth, occluder and articulator, skull, tables with muscles, base wax plates.
Questions for everyone.
Biomechanics is a branch of biophysics that in dentistry studies the movements of the lower jaw, the manifestations of the mechanical force of muscle contraction and the reaction of the teeth and periodontium to this force.
The concept of a functional system. The activity of the dental functional system is aimed at achieving a useful result - FORMATION OF A FOOD BALL.
Question 1. Let’s remember the structure of the dentition.
The teeth located in the jaws form dental arches.
The dental arch is a line drawn through the cutting edges and occlusal surfaces of the teeth near the vestibular contour.
The upper dental arch has the shape of a semi-ellipse, the lower – a parabola. The upper dental arch is slightly wider than the lower one, so the chewing surfaces of the upper teeth are located anterior and external to the lower ones.
In addition to dental arches, dentistry distinguishes alveolar and apical arches.
Alveolar arch is a line running along the edge of the alveolar process near the necks of the teeth on the vestibular side.
Apical arch - a line drawn along the tops of the roots of the teeth.
On the upper jaw, the crowns of the teeth are inclined towards the vestibular side, so the widest arch on the upper jaw is the dental one, and the narrowest is the apical one. The teeth of the lower jaw are inclined lingually, so the widest arch is apical, and the narrowest is occlusal.
The occlusal surfaces of the chewing teeth are not located in the same plane, but form the so-called sagittal occlusal curves.
The sagittal occlusal curve (curve of Spee) is a line passing through the buccal cusp of the first premolar and the distal buccal cusp of the last molar.
On the upper jaw the sagittal occlusal curve is convex, and on the lower jaw it is concave. Due to the presence of the curve of Spee, when lowering and moving the lower jaw forward, contact is maintained between the chewing teeth (the so-called Bonville three-point contact
).
Therefore, this curve is also called compensation
.
The plane passing through the incisal point on the lower jaw and touching the occlusal curves on the right and left is called occlusal.
In addition to the sagittal curve, there is also a transversal occlusal curve
. It is formed by tilting the upper molars to the buccal side, and the lower molars to the lingual side.
Transverse occlusal curve (Wilson curve) is a line passing through the occlusal surfaces of the chewing teeth of the right and left sides in the transverse direction.
The Wilson curve ensures contact of the dentition during transversal movements of the lower jaw. In the area of the first premolars there is no transverse occlusal curve.
Due to the presence of interdental contacts, the pressure during chewing is distributed to the periodontium of adjacent teeth. At the same time, the load on individual teeth is reduced. For optimal perception of chewing pressure by the jaw bones, according to the direction of the load, there are certain abutments (buttresses)
– bone thickenings through which the force of chewing pressure is transmitted to the cranial vault.
There are four buttresses on the upper jaw: frontonasal, alveolar-zygomatic, pterygopalatine
and
palatine
.
There are two buttresses defined on the lower jaw : alveolar
and
ascending
.
Temporomandibular joint. ARTICULATIO TEMPORO-MANDIBULARIS.
Question 5. Functions of the joint.
| Movement of the lower jaw | Movement in the temporomandibular joint |
| Down (mouth opening). | With a slight opening of the mouth - movement in the lower chamber of the joint (rotation of the head around the frontal axis); with wide opening of the mouth – displacement of the articular head and disc along the slope of the articular tubercle; with maximum opening of the mouth , the head rotates again around the frontal axis. |
| Up (teeth closing). | The movement is the opposite of the movement when opening the mouth. |
| Forward. | Movement in the upper chamber of the joint - sliding of the head together with the disc forward and down the slope of the articular tubercle; At the same time, there is a slight rotation of the head around the frontal axis. |
| Back. | Sliding of the articular head together with the disc back and up along the slope of the articular tubercle. |
| Right. | Right: movement in the lower chamber - rotation of the articular head around a vertical axis and shift of the head back and inward. Left: movement in the upper chamber - sliding of the head together with the disk forward and down, turning inward. |
| Left. | Right: movement in the upper chamber - sliding of the head together with the disk forward and down, turning inward. Left: movement in the lower chamber - rotation of the articular head around a vertical axis and shift of the head back and inward. |
6. Occlusion. Everyone remembers.
Occlusion is the position of the lower jaw in which a certain number of teeth are in contact.
There are four main types of occlusion: central, anterior, right lateral
and
left side
.
Question 8. Bite.
The nature of the closure of the dentition in the position of central occlusion is called occlusion
. A number of authors define occlusion also as a type of closure of the dentition in the usual position of the lower jaw. All types of bites are divided into physiological, pathological and abnormal.
To physiological
include bites that provide full chewing function, that is, bites in which multiple fissure-tubercle contact is observed (orthognathic, direct, prognathic, biprognathic and progenic types of bite).
Impairment of proper chewing due to abnormal
occlusion is caused by displacement of individual teeth or dentitions with the absence of multiple fissure-tubercle contact.
Abnormal types of occlusion include vertical incisal disocclusion
(“open bite”) and
sagittal incisal disocclusion
(extreme cases of “deep bite” and “progenic bite”).
With pathological
In the occlusion, multiple fissure-tubercle contact is absent due to the loss of one or more teeth.
In dental practice, an orthognathic bite is taken as the norm, so we consider the ratio of dentition for various types of occlusion for an orthognathic bite.
Lesson No. 5.
The structure and functions of the temporomandibular joint, the main muscles that carry out movements of the lower jaw in various directions, their functions. The structure of the dentition. Occlusion and articulation. Types of occlusion. Bite. Types of bite. Occlusiometry.
Required: film “biomechanics”, occluder with teeth, occluder and articulator, skull, tables with muscles, base wax plates.
Questions for everyone.
Biomechanics is a branch of biophysics that in dentistry studies the movements of the lower jaw, the manifestations of the mechanical force of muscle contraction and the reaction of the teeth and periodontium to this force.
The concept of a functional system. The activity of the dental functional system is aimed at achieving a useful result - FORMATION OF A FOOD BALL.
Question 1. Let’s remember the structure of the dentition.
The teeth located in the jaws form dental arches.
The dental arch is a line drawn through the cutting edges and occlusal surfaces of the teeth near the vestibular contour.
The upper dental arch has the shape of a semi-ellipse, the lower – a parabola. The upper dental arch is slightly wider than the lower one, so the chewing surfaces of the upper teeth are located anterior and external to the lower ones.
In addition to dental arches, dentistry distinguishes alveolar and apical arches.
Alveolar arch is a line running along the edge of the alveolar process near the necks of the teeth on the vestibular side.
Apical arch - a line drawn along the tops of the roots of the teeth.
On the upper jaw, the crowns of the teeth are inclined towards the vestibular side, so the widest arch on the upper jaw is the dental one, and the narrowest is the apical one. The teeth of the lower jaw are inclined lingually, so the widest arch is apical, and the narrowest is occlusal.
The occlusal surfaces of the chewing teeth are not located in the same plane, but form the so-called sagittal occlusal curves.
The sagittal occlusal curve (curve of Spee) is a line passing through the buccal cusp of the first premolar and the distal buccal cusp of the last molar.
On the upper jaw the sagittal occlusal curve is convex, and on the lower jaw it is concave. Due to the presence of the curve of Spee, when lowering and moving the lower jaw forward, contact is maintained between the chewing teeth (the so-called Bonville three-point contact
).
Therefore, this curve is also called compensation
.
The plane passing through the incisal point on the lower jaw and touching the occlusal curves on the right and left is called occlusal.
In addition to the sagittal curve, there is also a transversal occlusal curve
. It is formed by tilting the upper molars to the buccal side, and the lower molars to the lingual side.
Transverse occlusal curve (Wilson curve) is a line passing through the occlusal surfaces of the chewing teeth of the right and left sides in the transverse direction.
The Wilson curve ensures contact of the dentition during transversal movements of the lower jaw. In the area of the first premolars there is no transverse occlusal curve.
Due to the presence of interdental contacts, the pressure during chewing is distributed to the periodontium of adjacent teeth. At the same time, the load on individual teeth is reduced. For optimal perception of chewing pressure by the jaw bones, according to the direction of the load, there are certain abutments (buttresses)
– bone thickenings through which the force of chewing pressure is transmitted to the cranial vault.
There are four buttresses on the upper jaw: frontonasal, alveolar-zygomatic, pterygopalatine
and
palatine
.
There are two buttresses defined on the lower jaw : alveolar
and
ascending
.
The main muscles involved in the movements of the lower jaw.
THE POINTS OF ORIGIN AND ATTACHMENT OF MUSCLES MUST BE SHOWN ON THE SKULL!
Question 2. Masseter and temporal muscles.
- The chewing muscle itself. MUSCULUS MASSETER.
Begins: from the lower edge and inner surface of the articular arch, the anterior slope of the articular tubercle, the temporal fascia.
Attached: to the outer surface of the ramus of the lower jaw, to the masticatory tuberosity on the outer surface of the angle of the lower jaw, to the temporal tendon.
Function: raises the lower jaw, superficial layer – pushes the lower jaw forward.
— Temporalis muscle. MUSCULIS TEMPORALIS.
It begins: from the inner layer of the temporal fascia, from the platform of the temporal bone, from the temporal surface of the greater wing and the infratemporal crest of the sphenoid bone, parietal, scales of the frontal, temporal and temporal surface of the zygomatic bones.
Attached: to the coronoid process of the ramus of the mandible, to the ramus of the mandible in the area of the notch.
Function: Raises the lower jaw, the posterior fascicles pull the lower jaw pushed forward backward.