Jaw injuries are common in everyday life. However, a fracture of the upper jaw occurs much less frequently than a fracture of the lower jaw. The most common sources of such injuries are conflict situations involving physical violence and road traffic accidents. Injuries received at work or during sports training and competitions are also common. Maxillofacial trauma, accompanied by bone fracture, is very common in combat conditions.
A fracture of the upper jaw according to ICD-10 belongs to class S02.4, which is called Fracture of the zygomatic bone and upper jaw
Fracture of the upper jaw (appearance)
When exposed to traumatic factors on the maxillofacial area, the lower jaw most often suffers, since the splitting of the maxillary bone tissue requires a stronger mechanical impact. For example, the upper jaw can break when using brass knuckles, a stone, a hammer or other similar weapon in a fight. The cause of a fracture of the maxillary bone can also be a fall face-first onto concrete or stone, or a blow from a flying heavy body.
The specificity of a maxillary fracture is that it always has the character of breaking out a bone area, since the maxillary bone is rigidly connected to the adjacent cranial bones, and it is impossible to separate it from them without destroying the bone tissue.
Maxillary fractures are dangerous injuries leading to the loss of the jaw's supporting function. There is a risk of developing serious complications in the form of traumatic inflammation in the fracture area and additional injury to soft tissues from the sharp edges of the bone in the fracture area. In addition, with a maxillary bone fracture, even brain damage is possible - in particular, if it is accompanied by a fracture of the base of the skull. In such cases, in the absence of urgent measures, death can occur.
A blow to the jaw is the most common cause of jaw fracture.
With a strong mechanical impact on the upper jaw, as a rule, the facial area of the skull breaks into pieces. The fault lines run along the joints of the bones, the areas where the bone is thinnest, and the places where there are various functional openings through which blood vessels and nerve fibers pass. These natural holes weaken the mechanical strength of bone tissue, which is why fracture along them is most likely.
A fracture of the maxillary bone can cause serious negative consequences. Therefore, it is necessary to diagnose a bone fracture in a timely manner, and if it is detected, take immediate therapeutic measures. So, what are the types of maxillary fractures, how to identify them, and what measures should be taken to treat them?
Classification of fractures of the upper jaw
Maxillary bone fractures can be classified according to a general approach to dividing fractures into forms. In this context, the following forms of this type of injury are distinguished:
- Open fracture of the maxillary bone.
- Closed fracture of the upper jaw.
- Displaced jaw fracture.
- Fracture of the maxillary bone without displacement.
Classification of fractures of the upper jaw according to Lefort
The specific classification of maxillary fractures is based on the approach laid down by the French doctor Rene Le Fort, after whom the main types of fractures of the upper jaw are named, differing in the characteristic specificity of the split in the facial bone tissue. In accordance with this approach, the following injuries of the maxillary bone and the adjacent part of the face are distinguished:
- Le Fort fracture 1
- Le Fort fracture 2
- Le Fort fracture 3
Each of these fractures in a particular victim may have its own individual specifics. So, in particular, bone fragments can be displaced in the vertical or horizontal direction, and the shift directions for different fragments do not coincide in all cases. The severity of the patient's condition is determined by the position of the bone fracture line in height, as well as the weight and volume of the broken sections of the maxillofacial bone tissue.
What is a Le Fort 1 fracture?
This injury is an upper type of jaw fracture. This is the most severe maxillary injury, in which a fracture of the zygomatic bone and upper jaw occurs with their complete separation from the rest of the cranial bones. The contour of the face split goes from above along the natural orbital gaps, and from the side along the temporal bones. The median fracture hits the bone separating the nasal cavity from the cranial cavity and the intranasal septum. Against the background of this type of jaw fracture, there is always a fracture of the base of the skull.
Upper Le Fort can occur, for example, from blows delivered to the orbital area.
Maxillary fracture according to Le Fort 1, also known as the upper type of fracture (subbasal type)
What is a Le Fort 2 fracture?
Maxillary fracture Le Fort 2 (suborbital type)
With this injury, the fracture line runs almost along the boundaries of the maxillary bone mass, moving slightly, however, from the natural suture to the sides of the face or to its midline. This type of fracture is also called a suborbital fracture and is accompanied by damage to the nerves passing under the eye sockets. In rare cases, Le Fort 2 is complicated by a brain contusion, or a severe form of concussion, or a fracture of the cranial base.
What is a Le Fort 3 fracture?
With such an injury, the alveolar process breaks off and the nasal septum is destroyed. The split line runs along the nasal floor and maxillary sinuses. This type of fracture is accompanied by damage to the maxillary nerve ganglion. The consequence of this is a violation of nerve sensitivity in those areas of the face for which this plexus is responsible for transmitting impulses.
Maxillary fracture according to Lefort 3, also known as the lower type of fracture
All types of fractures of the upper jaw are very dangerous injuries, which is why it is so necessary to diagnose them in a timely manner and provide first aid. Therefore, it is very important to know the symptomatic picture when the integrity of the bones of the maxillary region of the face is violated.
Symptoms of a fracture of the upper jaw
The symptomatic picture of injuries to the maxillary bone, accompanied by its fracture, includes general signs of a fracture of the upper jaw, observed in any form of this injury, and symptoms characteristic of a specific type of jaw fracture.
The first sign of a fracture of the upper jaw bone is pain in the corresponding area of the face, which intensifies when trying to close the jaws. In addition, general symptoms in the case of a split maxillary bone are expressed in such signs as:
- Nose and mouth bleeding.
- Difficulty in nasal breathing.
- Vomiting - bone fragments located in the zone of excitation of the gag reflex are perceived by the nerve endings as a foreign object.
- Impaired vision and other sensory organs due to trauma to the eye sockets and a fracture of the base of the skull, leading to brain damage.
In addition to these general signs, there are also specific symptoms characteristic of each individual form of maxillary fracture.
Signs of a fracture of the upper jaw of the first type according to Le Fort
This type of damage is characterized by the largest size of bone tissue fragment and the longest split line length. A characteristic feature of this maxillary fracture is the leakage of cerebrospinal fluid from the nose and ears. When examined through the oral cavity, the flow of this fluid into the pharynx is also revealed. The reason for this is a fracture of the base of the skull.
When the upper jaw is broken according to the first type in Le Fort's classification, the following characteristic external manifestations occur:
- extensive swelling of the entire central area of the face and temple area;
- hemorrhages in the eye area, creating the visual impression that the patient was wearing dark glasses;
- the dependence of the shape of the face, the position of the eyes in the orbits and the relative position of the teeth of the upper and lower rows on the position of the victim’s body due to the mobility of bone fragments (when the patient lies, his face becomes flatter and his eyes deepen in the orbits, and when he stands or sits, his face becomes longer, the palpebral fissures widen, the eyes move downwards);
- double vision, increasing in a standing and sitting position, and decreasing in a lying position or when the jaws are tightly closed;
- upward displacement of the eyeballs when the mouth is tightly closed;
- lack of contact between the upper and lower teeth when closing the jaws;
- sagging of the soft palate, with the uvula in contact with the root of the tongue;
- sharp pain when opening the mouth.
Broken upper jaw - appearance
With a maxillary fracture, there are also neurological symptoms, namely:
- visual disturbances due to nerve injury, such as weakened vision, loss of its fields;
- the victim's inability to fully open their eyes;
- strabismus of convergent or divergent type;
- impaired sensitivity in the eye area.
With a type 1 jaw fracture, the patient has difficulty swallowing and constantly chokes. The reason for this is the sagging of the soft palate. Lowering the tongue to the root of the tongue leads to the sensation of a foreign body in the throat and provokes a gag reflex.
Symptom of glasses
The symptom of glasses is observed with a fracture of the base of the skull or upper jaw. Visually, with this symptom, you can notice the following changes on the face and in the general condition:
- red conjunctiva
- large bleeding into the skin (ecchymosis) in the area of the temporal bone of the injured side. The diameter of ecchymosis is at least 3-5 millimeters, irregular in shape.
- liquorrhea from the nose and ears
- nasal breathing disorder
- hearing impairment
- voluntary vibrations of the eyeballs (eye tremor - nystagmus)
- loss of creation
Symptom of glasses
The symptom can develop within a few minutes after the fracture, or after 12 or more hours. If this symptom is detected, emergency medical care must be provided immediately.
Symptoms of a Le Fort type 2 fracture of the upper jaw
With such a fracture of the maxillary bone, the following symptoms occur:
- nose and mouth bleeding;
- double vision;
- difficulty swallowing;
- difficulty breathing through the nose and mouth;
- feeling of a foreign object in the throat and gagging due to sagging of the soft palate;
- pain when clenching the jaws.
The specific symptomatic picture for this type of fractures includes the following manifestations:
- deterioration of the sense of smell or even its complete disappearance due to damage to the corresponding nerves;
- lacrimation, sometimes mixed with blood - due to deformation and damage to the lacrimal canal;
- impaired sensitivity of the facial skin in the area of the upper lip and nose, as well as under the eyes, manifested in the form of numbness;
- a feeling of stiffness in the area of the upper teeth and gums;
- extensive swelling of the face with accumulation of air in the tissues;
- hemorrhages in the area of the eye sockets and cheekbones;
- bulging of the conjunctiva even when the eyelids are closed due to hematomas and swelling in the eye area;
- protrusion of the eyes from the sockets above normal;
- increased pain when opening;
- hemorrhages in the tissue of the oral cavity;
- bulging of the pharyngeal walls due to hemorrhages in the corresponding area;
- the presence of a ledge in the area of the lower edge of the orbit that is detected by palpation.
As with a type 1 fracture, in the case of a type 2 fracture, there is elongation of the face in a vertical position and flattening in a horizontal position. Just as in the first version of the fracture, in the second there is incomplete closure of the teeth when closing the mouth - only the chewing teeth are in contact with each other. In some cases, the patient experiences a leak of cerebrospinal fluid - if the fracture of the upper jaw is accompanied by a fracture of the base of the skull.
Signs of type 3 upper jaw fracture
With this type of injury, a fracture of the maxillary sinus occurs, the alveolar process is broken off, as well as a split in the nasal septum. This is manifested by the following symptoms:
- painful sensations in the jaw, increasing when the mouth is tightly closed and attempts to chew;
- inability to use the front teeth to bite food;
- loss of sensitivity of teeth, gums and palate;
- malocclusion;
- difficulty breathing both through the nose and mouth;
- gagging due to the sensation of a foreign object in the throat;
- swelling of the lower area of the face, causing smoothness of the nasolabial folds;
- hematomas and enphysema in perioral tissues;
- an increase in the length of the lower third of the victim’s face when he stands or sits;
- shift of the nasal septum area upward when the dentition touches;
- bleeding into the oral mucosa.
Signs of a fracture, such as the presence of a ledge palpated at the site of the bone split, and a distortion of the bite, are not always detected in the case of a type 3 jaw fracture, but only in the presence of displacement.
Intraoperative complications
Fracture of the crown or root of the tooth being removed is most common . It is associated with significant damage to the tooth by the carious process, and sometimes depends on the anatomical features of the structure of the root and surrounding bone tissue. Often this complication occurs as a result of a violation of the surgical technique: incorrect application of forceps (failure to comply with the rule of coincidence of the axis of the cheeks with the axis of the tooth), insufficiently deep advancement, sudden movements during tooth dislocation, rough and incorrect use of elevators. In case of a tooth root fracture, it is necessary to continue the intervention using root forceps or a drill. Leaving the broken part of the root in the hole can lead to the development of an inflammatory process in the surrounding tissues. If for some reason (deterioration in general condition, technical difficulties, etc.) the broken root cannot be removed, the operation is completed, and the wound is sutured, if possible, or covered with iodoform turunda. Anti-inflammatory therapy and physiotherapy are prescribed. A repeat operation to remove the residual root is carried out after 7-14 days. By this time, inflammatory phenomena usually subside. A fracture or dislocation of an adjacent tooth can occur if this tooth is affected by caries or is not sufficiently stable and is used as a support while working with an elevator. If an adjacent tooth is fractured, it is removed. In case of dislocation, they are adjusted and a smooth splint-brace is applied for 3-4 weeks or a tooth replantation operation is performed (in case of complete dislocation).
Pushing the tooth root into soft tissue . Most often occurs during the removal of the third lower molar. This is facilitated by the resorption of the thin lingual wall of the alveoli as a result of a previous pathological process or its breaking off during an operation performed by an elevator. The dislocated root is displaced under the mucous membrane in the area of the maxillo-lingual groove. If the root located under the mucous membrane is palpable, then it is removed after cutting the soft tissue above it. When the removed root cannot be detected, an X-ray examination of the lower jaw is performed in frontal and lateral projections or CT and the location of the root in the soft tissues is determined. Topical diagnosis is aided by the insertion of needles into tissues followed by radiographs. The root, displaced in the tissue of the posterior part of the sublingual or submandibular region, is removed in a hospital setting.
Damage to the gums and soft tissues of the oral cavity occurs as a result of violation of the surgical technique and rough work of the doctor. If the circular ligament is not completely separated from the neck of the tooth, the gum connected to it may rupture during removal of the tooth from the socket. Applying forceps to the mucous membrane of the gum around the tooth “blindly” leads to its rupture. The prevention of this complication is the separation (flaking) of the gums to the middle of two adjacent teeth. Damaged soft tissues are sutured. Rupture of the soft tissues of the mouth can lead to bleeding. It is stopped by suturing the damaged mucous membrane. The crushed sections of the gums are cut off, and the torn sections are brought together with sutures. Fracture (fracture) of the alveolar process (part) of the jaw. Applying the cheeks of forceps to the edges of the socket is often accompanied by breaking off a small section of bone. This usually does not affect subsequent healing. Most often it is removed along with the tooth. If the broken section of bone is not separated from the socket along with the tooth, then it is separated from the soft tissue with a smoothing tool or a rasp and removed. The resulting sharp edges of the bone are smoothed. When elevators are used roughly when removing third molars, in some cases a separation of the posterior part of the alveolar process occurs, sometimes with part of the tubercle of the upper jaw. As a rule, the nonviable fragment is removed, the wound is sutured tightly or tamponed with iodoform turunda. TMJ dislocation . Its cause may be wide opening of the mouth and excessive pressure on the jaw with instruments during the removal of the lower small or large molars. The complication occurs more often in older people. Clinical picture: the patient cannot close his mouth. When palpating the heads of the condylar process, it can be determined that they have moved far forward beyond the slope of the articular tubercle. Their movements are significantly limited. Treatment consists of reducing the dislocation according to the standard technique described in the corresponding chapter.
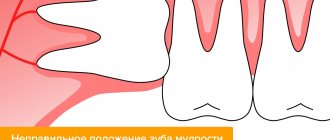
Prevention of dislocation is atraumatic tooth extraction and fixation of the lower jaw with the left hand during surgery to prevent wide opening of the mouth. Fracture of the lower jaw. This complication occurs extremely rarely. One of the main reasons is a violation of the wisdom tooth removal technique, when excessive force is used when removing it using a Lecluse elevator. Especially often, the risk of a fracture of the lower jaw arises if it is necessary to remove a tooth if there is a pathological process in the bone tissue in this area (radicular or follicular cysts, chronic osteomyelitis, jaw neoplasm, etc.). Osteopenic syndrome or osteoporosis is also important, especially in old age.
The clinical picture and treatment methods for a mandibular fracture are described in the corresponding chapter.
Perforation of the floor of the maxillary sinus is a common complication when removing upper molars or premolars. The cause of this complication may be the anatomical features of the structure of the maxillary sinus (close location of the roots of the teeth to the bottom of the sinus and a thin bony septum). A chronic inflammatory process in the periapical tissues (granuloma) leads to resorption of the bone septum, as a result of which the mucous membrane of the sinus becomes fused with the roots of the teeth and ruptures when removed. In this case, a communication occurs between the oral cavity and the maxillary sinus. Perforation of the bottom of the maxillary sinus can occur due to the doctor’s fault due to incorrect tooth extraction technique, when the specialist abuses the “pushing” movements of forceps, an elevator or a curettage spoon. If the bottom of the maxillary sinus is perforated, the doctor may feel a “sinking feeling”; sometimes blood with air bubbles is released from the hole. You can verify that perforation has occurred using careful probing or “nasal tests.” They consist in the fact that during exhalation through the nose, pinched with your fingers, air comes out of the hole with a noise or whistle.
Treatment of fractures of the upper jaw
The first steps in case of a maxillary fracture are first aid measures provided directly where the accident occurred. The victim’s body must be placed in a position in which pain is minimal. To prevent painful shock, the victim should be given an injection of an anesthetic. To prevent suffocation, the victim should be placed face down or on his side, and his head should be turned towards the area of injury.
Computed tomography: multiple injuries, diagnosis of fractures of the upper jaw
Pre-medical care for the victim also consists of eliminating bleeding, antiseptic treatment of open wounds and preparing him for transportation to the hospital, which includes fixing bone fragments with bandages.
The next step in treatment is establishing a diagnosis. For type 1 fractures, the diagnosis involves a surgeon and a neuropathologist, who identifies the neurological reactions inherent in this type of fracture.
The final diagnosis is made on the basis of an x-ray, which allows you to accurately determine the split line and the size of the bone fragments.
How is a jaw fracture treated?
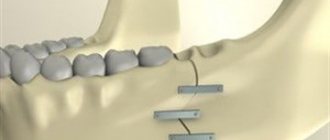
Treatment of fractures of the upper jaw: osteosynthesis with metal plates
Treatment of maxillary fractures is performed surgically. In the most severe cases, a complex operation is required to connect and fix bone fragments using wire sutures, as well as special titanium fasteners. When treating a maxillary fracture, it is important to prevent such undesirable consequences as:
- neurological and mental pathologies;
- circulatory and respiratory disorders;
- poor fusion of bone tissue masses;
- infection of the bone and adjacent tissues, leading to inflammation;
- the development of sinusitis and other diseases leading to the formation of a chronic source of infection in the body.
With a correct diagnosis and timely treatment, maxillary fractures have a favorable prognosis. Delay in taking therapeutic measures can cause various complications, in particular, improper fusion of fragments, requiring their fracture and subsequent reconnection.
First aid and treatment
If a fracture of the upper jaw is suspected, first aid at the scene of the incident consists of placing the body in the most gentle position in order to reduce pain and taking anti-shock measures (analgesics are required in any form, but preferably injectable).
Preventing asphyxia involves placing the patient face down or on his side with his head turned towards the wound.
Applying an aseptic dressing to the wound area helps stop bleeding and serves as a measure of protection against infection. If the injury is accompanied by chemical burns to the face, the remaining acid or alkali is washed off with water.
An immediate call for an ambulance or air ambulance, carried out in parallel with the provision of first aid, is all that a person on the street or a participant in the incident can help the injured person.
Providing full-fledged first aid consists of using anti-shock drugs, taking measures to stop bleeding and prevent asphyxia, and providing transport immobilization.
Subsequently, for fractures of the upper jaw, surgical methods of treatment or specialized emergency care are used in the department of maxillofacial surgery of a medical institution of a district or regional scale and includes surgical intervention to fix bone fragments for their subsequent consolidation.