I'm in honey!
Page content
Lower jaw, mandibula
Orientation: – chin protrusion facing forward; – the branch of the lower jaw is directed backward; - the alveolar arch is facing upward; – the masticatory tuberosity is directed laterally.
– large unpaired bone; consists of a body and two branches.
Body of the lower jaw, corpus mandibulae:
– base of the lower jaw, basis mandibulae. – lower, rounded edge; – alveolar arch, arcus alveolaris, – upper, rounded edge; – dental alveoli, alveoli dentales, – depressions in the arcus alveolaris for the roots of the teeth; – interalveolar septa, septa interalveolaria, separate the dental alveoli; – alveolar elevations, juga alveolaria, are protrusions on the outer surface corresponding to the alveoli; - chin protuberance, protubeirantia mentalis, located in the center of the basis mandibulae-, - chin tubercle, tuberculum mentale, - paired; limited on the sides by protuberantia mentalis; – the mental foramen, foramen mentale, is located lateral and superior to the proroluberanlia mentalis, (the vessels and nerve of the same name emerge); - mental spine, spina mentalis, - protrusion on the inner surface, behind the prorotuberantia mentalis - - sublingual fossa, fovea sublingualis, - paired depression on the sides of the spina mentalis - the salivary gland of the same name is located in it; – digastric fossa, fossa digastrica, steam room; located under/oued sublingualis-, weakly expressed; the muscle of the same name begins from it; - the maxillary-hyoid line, Ipea mylohyoidea, runs on the internal surface (the muscle of the same name is attached to it); - the submandibular cheeks, fovea submandibularis, is located under the previous line; adjacent to it is the salivary gland of the same name.
Branch of the lower jaw, ramus mandibulae
– the coronoid process, processus coronoideus, is a continuation of the branch anteriorly and upward;
– buccal ridge, crista buccinatoria, is located on the medial surface of the processus coronoideus; – condylar process, processus condylaris, ends with the head of the lower jaw, caput mandibulae; – the notch of the lower jaw, incisura mandibulae, is located between the processus coronoideus and the processus condylaris; – neck of the lower jaw, collum mandibulae, narrowed part of the processus condylaris; is under caput mandibulae; – pterygoid fossa, fovea pterygoldea, – a depression on the anterior part of the caput mandibulae (the lateral pterygoid muscle is attached to it); – opening of the lower jaw, foramen mandibulae, – located on the inner surface of the ramus mandibulae; – the tongue of the lower jaw, lingula mandibulae, limits the foramen mandibula on the medial side; – the canal of the lower jaw, canalis mandibulae, is a continuation of the foramen mandibulae; penetrates the body of the lower jaw and ends foramen mentale; – angle of the lower jaw, angulus mandibulae, – the place of transition of the posterior edge of the lower jaw branch into the base; – chewing tuberosity, tuberositas masseterica, located on the outer surface of the angulus mandibulae; – pterygoid tuberosity, tuberositas pterygoldea, is located on the inner surface of the angulus mandibulae.
Lower jaw: a – topography of the lower jaw; b – side view: 1 – coronoid process; 2 – notch of the lower jaw; 3 – pterygoid fossa; 4 – head of the lower jaw; 5 – condylar process; 6 – neck of the lower jaw; 7 – chewing tuberosity; 8 – angle of the lower jaw; 9 – base of the lower jaw; 10 – mental tubercle; 11 – chin protuberance; 12 – mental foramen; 13 – alveolar part; 14 – oblique line; 15 – branch of the lower jaw
Lower jaw. Front view.
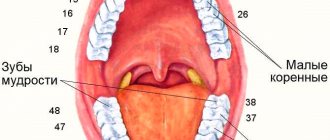
1 – alveolar eminences, 2 – coronoid process, 3 – condylar process, 4 – oblique line, 5 – masticatory tuberosity, 6 – angle of the lower jaw, 7 – mental foramen, 8 – subincisal depression, 9 – mental protuberance, 10 – body of the lower jaw, 11 – alveolar part, 12 – retromolar triangle, 13 – ramus of the lower jaw, 14 – pterygoid fossa, 15 – molars, 16 – premolars, 17 – canine, 18 – incisors.
Lower jaw, right half. Inside view. The left half of the lower jaw has been removed. 1 – buccal ridge, 2 – temporal ridge, 3 – notch of the mandible, 4 – head of the mandible, 5 – neck of the mandible, 6 – uvula of the mandible, 7 – opening of the mandible, 8 – mylohyoid groove, 9 – mandibular ridge, 10 – pterygoid tuberosity, 11 – maxillohyoid line, 12 – angle of the mandible, 13 – submandibular fossa, 14 – sublingual fossa, 15 – digastric fossa, 16 – compact substance of the mandible, 17 – spongy substance of the mandible, 18 – incisors, 19 – canine, 20 – premolars, 21 – molars.
Lower jaw, right half. Inside view. The left half of the lower jaw has been removed. 1 – buccal ridge, 2 – temporal ridge, 3 – notch of the mandible, 4 – head of the mandible, 5 – neck of the mandible, 6 – uvula of the mandible, 7 – opening of the mandible, 8 – mylohyoid groove, 9 – mandibular ridge, 10 – pterygoid tuberosity, 11 – maxillohyoid line, 12 – angle of the mandible, 13 – submandibular fossa, 14 – sublingual fossa, 15 – digastric fossa, 16 – compact substance of the mandible, 17 – spongy substance of the mandible, 18 – incisors, 19 – canine, 20 – premolars, 21 – molars.
Lower jaw. View from behind and below. 1 – head of the lower jaw, 2 – neck of the lower jaw, 3 – opening of the lower jaw, 4 – mylohyoid groove, 5 – angle of the lower jaw, 6 – mandibular ridge, 7 – upper mental spine, 8 – digastric fossa, 9 – lower mental spine , 10 – sublingual fossa, 11 – pterygoid tuberosity, 12 – lingula of the lower jaw, 13 – molars, 14 – premolars, 15 – canine, 16 – incisors. Lower jaw. Right and front view. The plate of compact substance has been removed. The mandibular canal is partially opened and a probe is inserted into it.
c – view from the inner surface: 1 – condylar process; 2 – coronoid process; 3 – tongue of the lower jaw; 4 – opening of the lower jaw; 5 – maxillary-hyoid line; 6 – mental spine; 7 – sublingual fossa; 8 – mylohyoid groove; 9 – mandibular ridge; 10 – pterygoid tuberosity; 11 – submandibular fossa; 12 – digastric fossa; 13 – angle of the lower jaw; 14 – neck of the lower jaw; d – top view: 1 – alveolar arch; 2 – retromolar fossa; 3 – temporal crest; 4 – coronoid process; 5 – tongue of the lower jaw; 6 – pterygoid fossa; 7 – head of the lower jaw; 8 – oblique line; 9 – mandibular pocket; 10 – base of the lower jaw; 11 – mental tubercle; 12 – chin protuberance; 13 – dental alveoli; 14 – interalveolar septa; 15 – mental foramen; 16 – interroot septa; 17 – neck of the lower jaw; 18 – condylar process; e – position of the opening of the lower jaw; e – value of the angle of the lower jaw
Lower jaw of an old man. View from above, right and front. 1 – pterygoid fossa, 2 – notch of the mandible, 3 – coronoid process, 4 – foramen of the mandible, 5 – retromolar fossa, 6 – alveolar part of the mandible, 7 – mental eminence, 8 – mental foramen, 9 – angle of the mandible, 10 – branch of the lower jaw, 11 – head of the lower jaw, 12 – neck of the lower jaw.
Extreme forms of the lower jaw: A – wide and short, B – narrow and long.
According to Gaivoronsky?
How about Prives?
- Osteology
Upper jaw
The upper jaw is a paired bone, the structure of which is much more complex in terms of anatomy than many other elements of the head skeleton. It is quite difficult to single out one important function of this part of the skull. With the help of this part of the skeleton, partitions between the nose and mouth are formed. Among other things, thanks to the upper jaw we are able to chew. Most of the bone is equipped with a mucous membrane. Experts call it the maxillary or maxillary sinus. If in animals we can observe the grasping function in the jaw area, then with humans everything is somewhat different. Because of this difference, our upper jaw is much smaller, and the ability to speak has made it even thinner. This part of the skeleton can be found in the upper anterior section. It is classified as an air-bearing bone.
This bone has its own four processes, as well as a body. The processes are called palatine and zygomatic, frontal and alveolar. The upper jaw (or rather its body) is created in an irregular shape. It is limited by four surfaces. It is slightly concave at the front. The body is separated from the orbital surface by the infraorbital margin. Under the latter, by the way, there is an infraorbital foramen. Both nerves and blood vessels pass through it. The middle edge at the anterior surface is equipped with a deep nasal notch. This in turn creates the anterior opening of the nasal cavity. Professionals call it the pear-shaped aperture. The part called the orbital surface does not have any roughness. Its shape resembles a regular triangle. The middle edge is equipped with a lacrimal notch. A lacrimal ossicle was found in its composition. The infraorbital groove originates not far from the posterior edge of the surface. After some distance, it passes into the infraorbital canal, which opens through the infraorbital foramen, located in the upper jaw.
The alveolar canals emerge from the infraorbital canal, through which nerves and vessels go to our front teeth. The zygomatic process is able to separate the anterior surface from the infratemporal one. The tubercle of the upper jaw is located in this part of the head skeleton. There are also alveolar canals here. Vessels and nerves pass through them. Just above the tubercle there is a large palatine groove. In turn, the nasal surface turns into the upper surface of the palatine process. In this part you can see the crest of the inferior turbinate. If you look at the reverse, that is, the back side of the frontal process, you can find a tear beard. Together with such elements as the inferior concha and the lacrimal ossicle they form the nasolacrimal canal. It helps connect the lower nasal passage and the orbit. At a distance from it there is a triangular opening, that is, the maxillary cleft. She will guide you to the maxillary sinus.
The frontal process extends from the body of the maxilla. He's going up. There, reaching a certain height, it comes into contact with the bow. On the side of the process there is an anterior lacrimal crest. It protects the tear groove in front. In the middle of it you can find a lattice ridge. On one side it is connected to the anterior part of the middle turbinate of the ethmoid bone.
The zygomatic process originates at the place where the facial and infratemporal, as well as the orbital surfaces of the body of the upper jaw intersect. The dimensions of the process are very relative. Its shape resembles a small but very wide protrusion. The zygomatic arch is created by connecting the process of the temporal bone, as well as the zygomatic process and the zygomatic bone itself.
The upper jaw also has an alveolar process. It originates from the upper jaw. In appearance it resembles a roller, that is, an alveolar arch. It has small depressions called dental alveoli. They contain the roots of eight teeth in half of the upper jaw. They are separated from each other by almost transparent bony partitions.
The bony palate is created by connecting the palatine process, as well as the process of the mandible and the posterior edge, with the horizontal plate of the palatine bone. This palate is considered the boundary for the nasal and oral cavities. The palatine process creates a large canal, which has a rather unusual U-shape. It is located behind the front teeth and incisors. Because of this, it received the name incisive. It originates from the upper jaw, in the place where the nasal surface is located. At a slight angle it passes through the palatine process. Then it passes through the midline and gradually turns into a furrow. Then the grooves, both on the right and on the left, turn into a single whole. Thus, a hole appears that opens on the midline of the bony palate.
Alveolar part and ramus of the mandible
The alveolar part of the body of the lower jaw contains 8 dental alveoli on each side. The alveoli are separated from each other by interalveolar septa (septa interalveolaria). The walls of the alveoli facing the lips and cheeks are called vestibular, and the walls facing the tongue are called lingual. On the surface of the body, the alveoli correspond to alveolar elevations (juga alveolaria), which are especially well expressed at the level of the canine and 1st premolar. Between the alveoli of the incisors and the mental protuberance there is a subincisal depression.
The structure of the alveoli of the lower jaw is similar to the structure of the alveoli of the upper jaw. The wall of the upper third consists of two layers: solid and compact plates (inner and outer). In the area of the bottom and lower third of the alveoli, under the hard plate there is a spongy substance.
The shape, depth and width of the alveoli, the thickness of their walls are different for teeth of different groups. The alveoli of the incisors (especially the central ones) are compressed from the sides, their bottom is shifted towards the vestibular compact plate, therefore the thickness of the lingual wall of the alveoli is greater than the vestibular one. The alveoli of the canine and especially the premolars are rounded, the lingual wall is thicker than the vestibular one. The deepest alveoli are at the canine and 2nd premolar. The thickness of their walls is greater than the alveoli of the incisors. The alveoli of molars have interradicular septa. In the alveoli of the first two molars there is one septum separating the anterior and posterior chambers for the corresponding roots. The alveolus of the 3rd molar has different shapes and a different number of septa, which is associated with the variability of the shape of this tooth. Most often the alveolus is conical, without septa, but may have one and sometimes two septa. The walls of the alveoli of the molars are thickened due to the oblique and mylohyoid lines. This strengthens the lower molars and protects them from loosening in the bucco-lingual direction during transverse (lateral) chewing movements.
The area of the jaw located behind the 3rd molar has the shape of a triangle and is called the retromolar fossa (fossa retromolaris). Laterally from this fossa, from the 2-3rd molar to the coronoid process, a mandibular recess (recessus mandibulae) stretches along the outer surface of the alveolar part, limited on the lateral side by an oblique line.
In the spongy substance of the body of the lower jaw there is a canal of the lower jaw (canalis mandibulae), through which blood vessels and a nerve pass. The canal begins with the opening of the lower jaw (foramen mandibulae) on the inner surface of the branch and ends with the mental opening on the outer surface of the body. The canal has an arcuate direction with a convexity facing down and forward, lies closest to the bottom of the alveoli of the 2-3rd molar and often passes between the chambers for their roots. Small tubules extend from the canal, through which vessels and nerves pass to the roots of the teeth; they open at the bottom of the alveoli. Medially from the mental foramen, the mandibular canal continues in the form of a small tubule to the midline and along this length gives off lateral branches to the bottom of the alveoli of the anterior teeth. In some cases, this tubule is absent, and then the vessels and nerves pass through the thickness of the spongy substance. In the region of the molars, the mandibular canal is located closer to the internal compact lamina, and in the region of the premolars it is adjacent to the outer compact lamina. Sometimes there is no spongy substance between the inner and outer plates at the level of the canal. In such cases, its walls touch the compact plates of the body of the lower jaw.
The branch of the lower jaw (ramus mandibulae) has outer and inner surfaces, anterior and posterior edges, which pass, respectively, into the coronoid process (processus coronoideus) and into the condylar process (processus condylaris). These processes are separated by the notch of the lower jaw (incisura mandibulae). The coronoid process serves to attach the temporal muscle, the condylar process serves to form the temporomandibular joint.
The condylar process has a head of the lower jaw (caput mandibulae) with an articular surface for connection with the mandibular fossa of the temporal bone and a neck (collum mandibulae). On the anteromedial surface of the neck of the lower jaw there is a pterygoid fossa (fovea pterygoidea) - the place of attachment of the lateral pterygoid muscle. The head of the lower jaw is flattened and occupies a position in which the axes drawn through the largest size of both heads intersect at the large opening at an angle of 120-180°, open anteriorly.
The anterior edge of the lower jaw branch passes downwards onto the outer surface of the jaw body in an oblique line. Along the medial surface of the coronoid process, from its apex, the temporal crest (crista temporalis) descends, to which the tendon of the temporal muscle is attached, and from its lower section the bundles of the buccal muscle begin. Below, the temporal crest bifurcates and, reaching the posterior alveoli, limits the retromolar fossa.
The posterior edge of the ramus of the lower jaw passes into the base of the jaw, forming an angle (angulus mandibulae) (see Fig. 1, e, art. Lower jaw), the value of which ranges from 110 to 145° (usually 122-133°).
The outer surface of the branch contains a masticatory tuberosity (tuberositas masseterica), which occupies most of the branch and the angle of the jaw and is the site of attachment of the masticatory muscle. On the inner surface of the branch in the area of the angle and adjacent sections there is a pterygoid tuberosity (tuberositas pterygoidea) - the place of attachment of the medial pterygoid muscle. On the same surface in the middle there is an opening of the lower jaw (foramen mandibulae), which is covered in front and above by an inconsistently pronounced bony protrusion - the tongue (lingula mandibulae). Above and anterior to the uvula is the mandibular ridge (torus mandibulae). The opening of the jaw is 10-25 mm from the anterior edge of the ramus, 9-20 mm from the posterior edge, 17-29 mm from the notch, 15-35 mm from the angle of the jaw (see Fig. 1, e, art. . Lower jaw). The smaller the angle of the jaw, the greater the distance from the angle. Most often, the opening of the lower jaw is located at the level of the chewing surface of the lower large molars, less often - above or below. In rare cases, this hole is double.
Ossification: The mandible develops as a pair of bones from connective tissue around cartilage. In the middle of the 2nd month of the intrauterine period, several ossification points appear on each side. Both bones fuse into one in the 2nd year of life.
Human anatomy S.S. Mikhailov, A.V. Chukbar, A.G. Tsybulkin
Published by Konstantin Mokanov
human anatomy
The upper jaw is a paired bone. It distinguishes between a body and four processes: frontal, zygomatic, alveolar and palatine.
The body of the upper jaw contains the air-bearing maxillary sinus (maxillary sinus), which communicates with the nasal cavity through the wide maxillary cleft. The body has an irregular shape; it has four surfaces: anterior, orbital, infratemporal and nasal. The anterior surface is concave. It is separated from the orbital surface by the infraorbital margin. Below this edge there is an infraorbital foramen through which blood vessels and nerves pass. Under this hole there is a depression - the canine fossa. On the medial sharp edge of the anterior surface, the nasal notch is clearly visible, participating in the formation of the anterior opening of the nasal cavity. The lower edge of the nasal notch projects anteriorly, forming the anterior nasal spine. The orbital surface forms the lower wall of the orbit and is a smooth triangular, slightly concave area. Its medial edge connects with the lacrimal bone, with the orbital plate of the ethmoid bone and with the orbital process of the palatine bone. In the posterior free part of the orbital surface, limiting the inferior orbital fissure, the infraorbital groove begins. Anteriorly, it turns into the infraorbital canal, which opens on the anterior surface of the upper jaw with the infraorbital foramen. The infratemporal surface participates in the formation of the infratemporal and pterygopalatine fossae; separated from the anterior surface by the base of the zygomatic process. The tubercle of the upper jaw is clearly visible on the infratemporal surface. Alveolar openings open on it, leading to the alveolar canals, through which nerves and vessels pass to the upper molars. Medial to the tubercle there is a vertically oriented greater palatine groove, which participates in the formation of the canal of the same name. The nasal surface has a complex topography, participates in the formation of the lateral wall of the nasal cavity, connects with the palatine bone, the inferior nasal concha and passes downwards into the upper surface of the palatine process of the upper jaw. On this surface, a triangular-shaped maxillary cleft is visible, in front of which there is a well-defined vertical tear groove. The latter, fused with the lacrimal bone and the inferior nasal concha, participates in the formation of the nasolacrimal canal. In front of this groove, across the base of the frontal process, there is a conchae crest, to which the inferior turbinate is attached.
The frontal process arises from the body of the maxilla at the point where the anterior, nasal and orbital surfaces meet. The upper serrated end of the frontal process reaches the nasal part of the frontal bone. On the lateral surface of the process, the anterior lacrimal crest runs vertically, continuing below into the infraorbital margin, which, together with the frontal process, limits the lacrimal groove in front. On the medial surface of the frontal process there is a ethmoidal crest with which the anterior part of the middle turbinate ethmoid bone fuses.
The zygomatic process arises from the superolateral part of the body of the maxilla. Its serrated end connects to the cheek bone.
The alveolar process is a thick plate, convex anteriorly and concave posteriorly, extending downward from the body of the upper jaw. The lower free edge of the process - the alveolar arch - has depressions - dental alveoli (sockets) for the eight upper teeth. The alveoli are separated from each other by interalveolar septa. On the outer surface of the alveolar process, alveolar elevations are visible, which are especially pronounced in the front teeth.
The palatine process has the appearance of a horizontal plate. It starts from the nasal surface of the body of the upper jaw, at the place of its transition into the alveolar process. The smooth upper surface of the palatine process participates in the formation of the lower wall of the nasal cavity. The medial free edge of the process carries an upwardly raised nasal ridge, which, together with the same ridge of the other palatine process, forms an elevation for connection with the lower edge of the vomer. The lower surface of the palatine process is rough; in the posterior part, palatine grooves oriented from back to front are noticeable. The medial rough edge of the palatine process, through a median suture, is connected to the process of the same name on the opposite side, forming the hard palate. At the anterior end of the median suture there is a hole leading into the incisive canal. The posterior edge of the palatine process connects to the horizontal plate of the palatine bone.
Like
Functions of the human upper and lower jaw
- Support function. The upper and lower jaw of a person serve as a support for the facial and chewing muscles. And there are many of these muscles; according to some reference books, a person has 57 separate muscles on the face alone.
- Protective function . The jaw bones protect the sensory organs and the upper digestive system.
- Digestion. Jaws are needed to bite and chew food. In addition, some muscles necessary for sucking and swallowing movements are attached to them.
- Breathing . The jaws serve as a container and support for the upper respiratory tract, in which air is filtered, humidified and heated.
- Speech. The jaws are involved in the process of articulation. Regulation of the opening of the mouth by the temporomandibular joint, the presence of teeth, the work of the muscles attached to the jaws - all this is necessary to make our speech intelligible.
- Facial expressions and communication. A movable lower jaw and facial muscles are necessary to reproduce emotions that are understandable to other people and communicate with the outside world.
INTERESTING: The mouth is the most developed part of the baby's body. This is where the most sensitive nerve endings are located, and therefore small children, in order to explore an object, pull it into their mouth.
Modern ideas about the normal anatomy and physiology of the temporomandibular joint and masticatory muscles will help the doctor establish the correct diagnosis and outline rational methods of treating various diseases of this joint.
The temporomandibular joint (articulatio temporo-mandibularis) is the functional center of the masticatory apparatus. This is a paired, combined, incongruent joint formed by the head of the mandible (caput mandibulae), the mandibular fossa (fossa mandibularis), the articular tubercle of the temporal bone (tuberculum articulare), . articular disc (discus articularis) and joint capsule (capsula articularis) (Fig. 1).
Rice.
1. Temporomandibular joint (according to V.P. Vorobyov and R.D. Sinelnikov, 1946). 1—suetaz capsule; 2 - retroarticular tubercle; 3 - mandibular fossa; 4 - articular disc; 5 - articular tubercle; 6 - upper head of the lateral pterygoid muscle; 7 - lower head of the lateral pterygoid muscle; 8 - infratemporal crest; 9 - tubercle of the upper jaw; 10 - coronoid process; 11 - branch of the lower jaw; 12 — notch of the lower jaw; 13 - stylomandibular ligament; 14 - styloid process; 15 - head of the lower jaw; 16 - external auditory canal. Intracapsular ligaments fix the articular disc to the temporal bone and to the inner and outer surfaces of the neck of the lower jaw [Kudrin I. S., 1968].
In addition, the temporomandibular joint includes the lateral ligament (lig. laterale), sphenomandibular ligament (lig. sphenomandibulare), stylomandibular ligament (lig. stylomandibulare) (Fig. 2).
Rice. 2. Ligaments of the lower jaw (according to V.P. Vorobyov and R.D. Sinelnikov, 1946). 1 - joint caggsula; 2 - sphenomandibular ligament; 3 - stylomandibular ligament; 4 - pterygospinous ligament; 5 - pterygoid process; 6 - lateral pterygoid muscle.
Movements in this joint are performed by the masticatory (m. masseter), temporal (m. temporalis), medial pterygoid (m. pterygoideus medialis), lateral pterygoid (m. pterygoideus lateralis), mylohyoid (m. mylohyoideus), digastric (m. digastricus), geniohyoid (m. geniohyoideus) muscles. The listed anatomical formations of the temporomandibular joint take an active part in all movements of the lower jaw during chewing, swallowing, talking, laughing, coughing, etc. At the same time, the muscles of the tongue and facial muscles are involved in this.
Various movements of the lower jaw are carried out by the highly coordinated activity of all elements of the temporomandibular complex and, above all, by the activity of the masticatory muscles, regulated by the nervous system. Let's consider the anatomical structure of the elements of the temporomandibular complex.
The head of the lower jaw is shaped like a roller curved in the frontal plane, up to 20 mm long and up to 10 mm wide.
In the anterior superior part of the head there is an articular surface. In adults, the rhinum is covered (like the articular surface of the posterior slope of the articular tubercle) with fibrous cartilage. The perichondrium of the articular surfaces of the joint passes into the periosteum of the bones that form the joint [Nesvizhsky S. O., 1950]. The head of the mandible is under the influence of muscles.
There are different opinions regarding its position in the glenoid fossa. The Zurich Orthopedic School considers the correct position of the head in the deepest part of the articular fossa. According to the German school, the normal position of the head is at the posterior slope of the articular tubercle. However, observations by Reichenbach E. (1970) showed that there is no specific position of the head; moreover, the rule is the absence of any pattern in its location.
The position of the head during physiological rest depends on muscle tone, and in case of central occlusion - on the intermaxillary relationship of the teeth. When teeth are lost, the head of the lower jaw usually moves more upward and posteriorly. In this position, it can put pressure on the tympanic part of the temporal bone, causing a number of painful conditions [Kurlyandsky V. Yu., 1977].
Mandibular fossa
The mandibular fossa is bounded in front by the articular tubercle, in the back by the squama of the temporal bone, on the outside by the base of the zygomatic process of the temporal bone, and on the inside by the angular spine, its arch is separated from the middle cranial fossa by a thin plate of compact bone. The absolute depth of the mandibular fossa in adults ranges from 7.2 to 11 mm. With the loss of teeth, the articular tubercle atrophies and the depth of the fossa decreases [Bregadze G.V., 1951]. Newborns already have a functioning joint, but the mandibular fossa is practically absent.
The mandibular fossa serves as a container for the head of the lower jaw when the teeth are closed. It is not a functioning component of the temporomandibular joint, therefore there is no cartilaginous cover in the deep parts of the fossa. It is present only on the posterior slope of the articular tubercle (Fig. 3).
Rice. 3. The location of the cartilaginous cover on the functioning surfaces of the head of the mandible and the posterior slope of the articular tubercle - 4 (shaded in black) (Scgwartz L., 1959). 1 - head of the lower jaw; 2 - mandibular fossa; 3 - articular tubercle.
Articular tubercle
The articular tubercle in adults is represented by an ellipsoidal protrusion located in the lower part of the zygomatic process of the temporal bone. The anterior surface of the articular tubercle faces the infratemporal fossa, the posterior surface is the articular surface along which the head of the mandible moves. The height of the articular tubercle ranges from 5 to 25 mm. The angle of inclination of the posterior slope of the articular tubercle to the Frankfurt horizontal is in the range of 48° - 90° [Mikheev V.G., 1975]. The bony surfaces of the articular tubercle and the head of the lower jaw facing the joint cavity are convex and incongruent.
P.M. Egorov, I.S. Karapetyan