Worn teeth can be present not only in older people. There is such a thing as pathological tooth abrasion, which is a pathological process characterized by intense loss of hard tissue in all teeth and in one. This phenomenon occurs in slightly more than 10% of people. Most often, it affects men after 30 years of age.
Physiology is to blame for everything
To begin with, let's say that all the causes of tooth wear can be divided into two large classes - physiological and pathological.
The first reason appears immediately after the final eruption of baby teeth - and this is a natural process. In children, the incisors, cusps on the canines and molars gradually wear away, and by the age of 6 years, the depth of wear down to the dentin can be observed. In the future, until the age of 14, when the teeth are finally replaced by permanent ones, abrasion of the dentinal layer of the first teeth is sometimes noted. Severe abrasion is diagnosed when the entire upper part of the tooth disappears or the cavity becomes visible.
In general, due to physiological characteristics, teeth adapt to stress during the process of wear. Without dangerous overloads, the work of the entire dental system is adjusted; contacts between teeth change the angle from point to plane, so that the closure of the jaws is more physiological.
If the changes affect only the enamel, there is nothing to worry about. But if dentin begins to participate in the process of abrasion, this is a reason to consult a doctor.
Treatment of worn teeth
Today, there are many ways to restore teeth that are subject to significant wear. It all depends on the nature of the pathology, the skills and abilities of the specialist.
Important! The key factor in treatment is to diagnose as accurately as possible, correct problems that lead to increased wear, followed by restorative treatment using direct and indirect restoration techniques.
Identification and elimination of the etiology of the disease The first issue that arises in the treatment process is the identification of etiological factors and their elimination. The purpose of this stage is to remove those areas that are subject to increased load. They can cause pain in the patient, preventing normal jaw movement.
How is pathology determined?
Only a specialist can detect a violation during tooth wear. Of course, the general picture among the population is taken as the norm, but the doctor also takes into account individual factors:
- general condition of the enamel;
- presence or absence of exposed dentin;
- work of the temporomandibular joint;
- condition of the mucous membranes of the tongue and cheeks;
- degree of severity of nasolabial folds;
- sensitivity of the masticatory muscles.
It is interesting that in addition to all the individual characteristics, the doctor is interested in the sound with which the jaws close. A sharp, clear and short sound indicates that there are no problems. A long-lasting sound accompanied by a squeak indicates deficiencies in the functioning of the TMJ or problems with the nervous system.
You can understand that teeth are subject to increased abrasion by the first sign - increased sensitivity. It is sharper when the upper hard layer of enamel is significantly abraded.
Patient examination plan
Traditionally, the examination begins with getting to know the patient, collecting anamnesis and complaints. At this stage, the doctor finds out when the disease began, how it manifests itself, what it may be associated with (the patient’s lifestyle, previous treatment, harmful occupational factors, etc.). If the problem has just begun to manifest itself, then complaints as such may be absent or only slightly expressed. Typically, patients note discomfort when eating hot and cold food, chipping of the enamel or its thinning, and changes in diction (in later stages of the disease).
At the next stage, the doctor proceeds to examine the oral cavity, during which he evaluates:
- Bite.
- Overlapping of incisors.
- The shape of the dentition.
- The shape of the teeth.
Based on the data obtained, the doctor can prescribe additional research methods (radiography, MRI, electroodontodiagnostics, etc.), as well as consultations with more specialized specialists.
Modern and classic classification of abrasion
In modern Russian practice, the most widespread and popular is the Bushan classification of abrasion, which distinguishes:
✔
physiological abrasion (only enamel is affected);
✔
transitional (enamel + dentin suffers);
✔
pathological abrasion (dentin is damaged).
The benefit of the classification is that, in addition to the degree of pathology, it considers the surfaces (vertical, horizontal) that have undergone changes, the prevalence of the disease and the tooth sensitivity accompanying the process.
As for the types of pathological abrasion, the classical classification was developed by A. G. Moldovanov and L. M. Demner. According to their data, the rate of abrasion is 0.402 mm per year.
- The first degree of abrasion
is achieved by the age of 25-30 and is characterized by smoothing of the cusps and cutting edges of the teeth. - The second degree of abrasion
is observed in patients aged 44-50 years and is expressed in the abrasion of the enamel. - The third degree of abrasion
is noted if by the 50th anniversary the enamel limit has been reached and 10 pairs of chewing teeth have been preserved.
Increased tooth wear (pathological tooth wear)
Classifications of pathological tooth abrasion Bracco's classification The Bracco classification is the most widely used. He distinguishes 4 degrees of abrasion: 1. Erasure of the enamel of the cutting edges and tubercles. 2. Complete erasure of the cusps up to 1/3 of the crown height with exposure of dentin. 3. Reducing the crown height to 2/3. 4. The process spreads to the level of the tooth neck.
Classification by A.L. Grozovsky A.L. Grozovsky (1946) identifies three clinical forms of increased tooth abrasion: 1. Horizontal 2. Vertical 3. Mixed
Classification by V.Yu. Kurlyandsky During the pathological process, V.Yu. Kurlyandsky (1962) distinguishes between localized and generalized forms of increased abrasion.
Classification by M.G. Bushana The classification proposed by M.G. is considered to be one of the most fully reflective of the clinical picture of tooth abrasion. Bhushan (1979). It includes various clinical aspects of a functional and morphological nature: stage of development, depth, extent, plane of the lesion and functional impairment.
Depth of tooth damage I degree - complete dentin exposure and shortening that does not reach the equator (within 1/3 of the length of the tooth crown); II degree – shortening from 1/3 to 2/3 of the crown length; III degree – shortening of the tooth crown by 2/3 or more
Development stage I (physiological) – within the enamel; II (transitional) – within the enamel and partially dentin; III (increased) – within dentin
Damage plane I – horizontal; II – vertical; III – mixed
Length of lesion I – limited (localized); II – generalized
Classification by A.G. Moldovanova, L.M. Demner The most modern classification of increased and physiological abrasion of permanent teeth can be considered the classification proposed by A.G. Moldovanov, L.M. Demner (1979). Long-term clinical studies and observations have shown that with an optimal course of physiological abrasion, the natural loss of hard dental tissues per year ranges from 0.034 to 0.042 millimeters.
Studies have also shown that abrasion within the enamel-dentin boundary at the age of 50 years and older with a preserved dentition, in which there are at least 10 pairs of antagonist teeth, is a natural process.
Based on this, the authors came to the conclusion that physiological abrasion of teeth has its own forms of abrasion: 1. Form I - abrasion of the incisor teeth and smoothing of the cusps of molars and premolars (up to 25-30 years). 2. Form II - abrasion within the enamel (up to 45-50 years). 3. III form - abrasion within the enamel-dentin border and partially dentin (50 years and older).
Classification of increased abrasion of hard tissues of teeth includes localized and generalized increased abrasion of hard tissues: 1. I degree - in the areas of enamel, partially dentin. 2. II degree - within the main dentin (without transillumination of the tooth cavity). 3. III degree - within the replacement dentin (with transparency of the tooth cavity). 4. IV degree - abrasion of the entire tooth crown. Forms of abrasion: horizontal, vertical, facet, lattice, stepped, cellular, mixed.
Classification by A.G. Moldovanov As a result of the research, A.G. Moldovanov (1992) proposed a classification of increased and physiological abrasion of primary (temporary) teeth.
Physiological abrasion of hard tissues of temporary (baby) teeth: 1. By the age of 3-4 years of a child’s life, the teeth of the incisors and the cusps of the canines and molars wear out (I form). 2. By the age of 6 - abrasion within the enamel layer, up to a point opening of the enamel-dentin border (II form). 3. Over 6 years - abrasion within the dentinal layer of teeth before replacement with permanent teeth (III form).
Increased abrasion of hard tissues of temporary (baby) teeth: 1. Translucency of the tooth cavity (IV form). 2. Abrasion of the entire tooth crown (V shape).
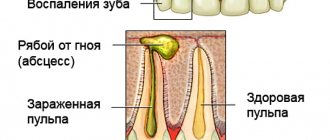
With pathological abrasion of teeth, abrasion of enamel and dentin is observed, and after dentin is exposed, abrasion occurs more intensely, since dentin is a softer tissue. As a result, sharp edges of the enamel are formed, which often injure the mucous membrane of the cheek and lips. If treatment is not carried out, the wear progresses quickly and the tooth becomes significantly shorter. In such cases, there are signs of a decrease in the lower third of the face: folds at the corners of the mouth, changes in the temporomandibular joint, pain in the temporomandibular joint and tongue, and decreased hearing.
With the initial manifestations of pathological abrasion of teeth, sensitivity to temperature irritations appears, and as the process deepens, pain from chemical and mechanical irritations appears.
As the cusps of the chewing surface wear off with age, the wear on the incisors progresses intensively. The length of the incisor crowns decreases and by the age of 35-40 decreases by 1/3-1/2. Instead of a cutting edge, significant areas are formed on the incisors, in the center of which dentin is visible. Once dentin is exposed, it wears off more intensely than enamel, resulting in the formation of sharp edges that injure the cheeks and lips. If treatment is not carried out, tissue abrasion progresses rapidly, and the crowns of the teeth become significantly shorter. The lower third of the face decreases, which is manifested by the formation of folds at the corners of the mouth. In persons with a significant decrease in bite, changes in the temporomandibular joint may occur and, as a result, burning or pain in the mucous membrane, hearing loss and other symptoms characteristic of low bite syndrome may occur. With further progression of the process, the abrasion of the incisors reaches the necks. The tooth cavity is visible through the dentin, but it is not opened due to the deposition of replacement dentin. In a deep bite, the labial surface of the lower incisors comes into contact with the palatal surface of the upper incisors and these surfaces are significantly worn away. The most pronounced tissue abrasion is observed in the absence of part of the teeth. For example, in the absence of molars, on which the relationship of the dentition normally depends, the incisors and canines are intensively worn out, as they are overloaded. In addition, due to overload, displacement of teeth and resorption of bone tissue at the apexes of roots and interdental septa may occur. Often, tooth wear is caused by improper design of removable and fixed dentures. When using a tooth under a clasp without an artificial crown, the enamel and dentin at the neck are often erased. As a rule, patients complain of severe pain when exposed to mechanical and chemical stimuli. As is known, the specific conditions of some industries are the cause of occupational diseases. In a number of industries, teeth are damaged and frequently worn out. In workers engaged in the production of organic and, especially, inorganic acids, examination reveals more or less uniform abrasion of teeth of all groups; there are no sharp edges. The surfaces of the teeth have a matte tint, there is no plaque. In some places exposed dense smooth dentin is visible. In people with extensive experience working in acid production plants, the teeth are worn down to the neck. One of the first signs of enamel abrasion under the influence of acid is a feeling of teeth on edge and roughness of the surface of the teeth. The change from a feeling of soreness to pain indicates the progression of the process. The chewing process may be disrupted. Upon examination, a loss of the natural color of the tooth enamel is revealed, which is especially visible when dried. The waviness of the enamel surface may be slightly expressed. People who work in enterprises where there are excess mechanical particles in the air also experience increased tooth wear.
Often, increased tooth abrasion occurs in a number of endocrine disorders - dysfunction of the thyroid, parathyroid glands, pituitary gland, etc. The abrasion mechanism in this case is due to a decrease in the structural resistance of tissues. In particular, increased abrasion is found in fluorosis, marble disease, Capdepont-Stainton syndrome, primary underdevelopment of enamel and dentin.
Causes of pathological abrasion
There are several main reasons for the development of abrasion pathology, and in the first place among them are bad human habits. For example, the habit of gnawing seeds, holding small objects in the mouth (pins, cloves, pipe mouthpiece), love for foods with high acidity may well become catalysts for the process.
Often the cause of increased abrasion is diseases: bruxism, diseases of the gastrointestinal tract, nervous, cardiovascular, endocrine systems, from the side of the TMJ - malocclusion. The cause may also be improper dental treatment - an incorrectly manufactured orthopedic design can provoke severe abrasion of the antagonist tooth.
Sometimes the cause of pathology may be the chosen profession. Some employees of the metallurgical, cement, granite industries, and representatives of the mining workshop suffer from increased abrasion.
Treatment and prevention of enamel wear
It is very important to stop the progression of the pathology, and for this the doctor must find out the individual reasons for its occurrence. To restore the anatomical shape of already worn-out crowns, veneers, inlays, and crowns are used. To increase the height of the bite, filling is performed with metal ceramics or photopolymers.
If one or more teeth are missing, it is advisable to undergo dental implantation or removable dentures.
If you have an incorrect bite, you should definitely undergo full orthodontic treatment (as a rule, vestibular braces are used for this). If you are worried about bruxism, then everything is much simpler - the dentist will make a special mouthguard that you will need to wear at night.
If there is an increased effect of acid on the enamel, it is recommended to rinse the mouth with a soda solution.
The best prevention of increased enamel wear is proper nutrition, giving up bad habits and, of course, regular dental checkups. You can choose a competent specialist on our website. We have collected a complete database of dentists.
Treatment
Treatment of pathological tooth abrasion is carried out by orthopedists or dental therapists. The main efforts of specialists are aimed at eliminating the etiological causes of pathological tooth abrasion, normalizing occlusion, and restoring hard tissues.
To eliminate the causative factors, correction of mineral metabolism processes and treatment of endocrine pathologies are carried out. It is advisable to change some habits (open bottles with your teeth, chew hard foods, etc.), install dentures if some teeth are missing, or replace them if the old ones were made poorly. To combat hyperesthesia, complex remineralizing therapy is also prescribed. It includes:
- taking mineral and vitamin complexes;
- applications with fluoride-containing drugs;
- electrophoresis.
If worn teeth have sharp edges that can injure soft tissues, they are polished.
If you suffer from bruxism, you may need to wear a night guard. In some cases, the doctor may recommend closing the end defects of the teeth using bridges or partially removable dentures. This article will tell you what to do if your teeth begin to crumble.
A mouthguard for bruxism should be made individually, in accordance with the shape of the dentition.
In principle, restoration with filling materials, artificial crowns, core inlays, lumineers and veneers is used for similar purposes. Please note that pathological abrasion is often associated with bite defects and requires preliminary adjustment of the bite before prosthetics.
Treatment provided in the clinic
After a mandatory comprehensive examination of the oral cavity, establishing the condition of the tooth enamel and pulp, the doctor immediately begins treatment, while the destruction process can still be stopped.
Treatment takes place in several stages:
- general sanitation of the oral cavity: treatment of existing caries, removal of tartar, elimination of possible inflammation of the mucous membrane;
- areas of tooth enamel that are susceptible to abrasion are treated with compounds containing calcium salts - this strengthens the hard shell of the tooth and is called
- introduction of enamel-strengthening compounds and solutions through electrophoresis - this is how the healing elements penetrate deeper into the tooth and treat it from the inside;
- stopping further erosion of tooth enamel using orthopedic techniques: temporary plates, crowns or dentures are placed on the teeth to increase the height of the teeth.
High-quality prostheses are used: cast, porcelain or very reliable and environmentally friendly plastic. If there is partial loss of teeth, then removable temporary dentures to combat increased abrasion are combined with fixed ones, which will serve you for many years and will not cause any discomfort at all.
Sawing technique
The process of grinding teeth is carried out in several stages.
Preparation
At the dentist's appointment, the condition of the jaw row units is assessed. The doctor determines the possibility of filing hard tissues or identifies contraindications to the procedure. Using copying material and a liquid aerosol, he marks those parts of the tooth that will be ground down in the future.
Sawing
This procedure has several techniques, depending on the final goal, as well as the shape of the teeth. When working with chewing molars, the doctor carefully files the outer layer of enamel. And when grinding down the front incisors, the dentist works with the device in different directions.
In some situations, it may be necessary to preliminary produce a diagnostic model based on the example of a cast of the patient’s dental units. The finished plaster sample is thoroughly studied and subject to grinding.
Carborundum cutters or diamond burs are used as tools for the event.
On this topic
- Restoration
What is skyce in dentistry?
- Maria Konstantinovna Tevs
- September 30, 2020
The procedure of filing teeth usually ends with polishing and remineralization. The specialist applies a substance to the enamel that contains a complex of useful elements that increases the strength of bone tissue and increases its density.
Some people believe that the filing procedure is not technically difficult and try to do it at home on their own. Based on this experience, patients often end up in the hospital with damaged enamel and decayed teeth.
Dentists strongly recommend performing the event only with the help of a specialist and within the walls of a medical institution in order to avoid any negative consequences. In addition, the following phenomena are often observed as a result of self-medication:
- Large cracks in hard tissue.
- Damage to dentin caused by penetrating bacteria.
- Infectious infections.
- Pulpitis.
- Complete loss .