April 18, 2020 Last revised: December 18, 2020 Oral diseases
What to do if a patient is suddenly diagnosed with actinomycosis of the oral cavity? On medical websites you can find information that some forms of actinomycosis can be fatal for patients. is it so bad? What health problems are meant by this term, why does it occur, by what signs can this disease be suspected, and is it really possible to completely cure maxillofacial actinomycosis? How serious and inevitable are the complications of actinomycosis, and what measures with the greatest effect will help protect against this chronic disease, prone to relapses? We invite you to learn about all this in our article.
Description of the disease
Actinomycosis is an infectious disease that can affect the skin and internal organs of a person. This disease has a chronic course with a tendency to relapse and occurs due to the entry of actinomycetes into the body.
With this disease, granulomatous lesions appear in various organs. In most cases, actinomycosis primarily affects the maxillofacial area. The causative agent of actinomycosis is well known - it is the “human radiant fungus”. Actinomycetes are quite common in nature; they can also often be found in the body of healthy people. Often these microorganisms are found in a person’s mouth and gastrointestinal tract.
Features of the treatment of actinomycosis
| Figure 1. Actinomycosis of the maxillofacial region. Stage of fistula. |
| Figure 2. Actinomycosis of the mammary gland. |
Actinomycosis, according to various sources and classifications, is also called deep mycosis, pseudomycosis, actinobacteriosis, radiant fungal disease, etc. This disease is distinguished by a variety of clinical manifestations, which is associated with the stage of development of a specific process (infiltrate, abscess formation, fistula formation, scarring) and with its numerous localizations (head, neck, ENT organs, chest, lungs, mammary gland, axillary and inguinal areas, abdominal wall, liver, intestines, genitals, cecum, buttocks, limbs, etc., Figures 1, 2, 3, 4).
Judging by some publications and medical reports, it can be noted that there are certain discrepancies in the understanding of the etiopathogenesis of actinomycosis and the role of actinomycetes in the development of chronic purulent diseases. And knowledge of the etiology of the disease, as is known, is especially important when choosing etiotropic treatment.
Actinomycetes (microaerophilic, aerobic and anaerobic microorganisms) are widespread in nature; they live in soil, on plants, in water, on stones, in residential and industrial premises, and are also constantly present in the human body. An important diagnostic sign of actinomycosis is the detection of actinomycetes during cultural examination of pathological material and/or drusen of the radiant fungus, which are radiate formations - thickened filaments of mycelium with characteristic “cones” at the end (Figure 5).
| Figure 3. Thoracic actinomycosis. Damage to the soft tissues of the axillary region, chest wall and lungs. |
| Figure 4. Actinomycosis of the inguinal and suprapubic areas involving the pelvic tissue. |
In the 30-40s. XIX century actinomycetes (radiant fungi) were considered microorganisms occupying an intermediate position between fungi and bacteria. The ability of actinomycetes to form aerial mycelium, their lack of organs of fruiting, differentiation, and cellular vegetation bring them closer to true mushrooms. However, in terms of the chemical composition of their shells, protoplasm, and DNA structure, actinomycetes correspond to bacteria. It has been definitively proven that the causative agents of actinomycosis—actinomycetes—are bacterial cells.
In most cases (70-80%), actinomycosis develops under the combined influence of actinomycetes and other bacteria that secrete enzymes (including hyaluronidase) that melt connective tissue and contribute to the spread of the actinomycotic process.
The entry gates for actinomycetes and other bacteria into the body (exogenous route) are damage to the skin, mucous membranes, microtraumas, cracks, sockets of extracted teeth, congenital fistulous tracts (branchiogenic, salivary, umbilical, embryonic ducts in the coccygeal region), etc.
An important role in the pathogenesis of actinomycosis belongs to endogenous: hematogenous, lymphogenous and contact routes of penetration of microorganisms.
The development of actinomycosis of various localizations is usually preceded by various types of trauma, bruises, traumatic extraction of teeth, especially the 8th dystopic tooth, jaw fracture, chronic periodontal disease, periapical granuloma, shrapnel wounds, prolonged riding of a motorcycle, bicycle, perineal rupture during childbirth, intrauterine devices, hemorrhoids, anal fissures, sacrococcygeal cysts, the presence of chronic inflammation: appendicitis, adnexitis, paraproctitis, hidradenitis suppurativa, sycosis, acne, tonsillitis, osteomyelitis, etc.
| Figure 5. Actinomycotic drusen (histological specimen). |
| Figure 6. Surgical excision of the focus of actinomycosis in the sacrococcygeal region. Partial suturing of the wound. |
| Figure 7. Fistulography: when a contrast agent is introduced into the fistula, branched fistula tracts are visible on the anterior abdominal wall. |
At the site of introduction of actinomycetes at the first stage of the disease, a specific granuloma is gradually formed, without visible clinical symptoms and subjective complaints - actinomycoma, consisting of leukocytes, giant cells, infiltrative tissue, microabscesses, granulations, proliferative elements, connective tissue bridges and the surrounding capsule.
Actinomycosis is a chronic purulent non-contagious disease that affects people of working age and without adequate treatment can last for years; the disease tends to progress. The formation of chronic inflammation and specific granulomas with subsequent abscess formation and the formation of fistulous tracts in visceral localizations aggravates the patient’s condition and leads to dysfunction of the affected organs, the development of anemia, intoxication and the appearance of amyloidosis.
Actinomycosis and other bacterial infections of the craniofacial and visceral localization require complex treatment - the prescription of anti-inflammatory, immunomodulatory, restorative drugs, the use of surgical and physiotherapeutic methods. Treatment of severe forms of visceral actinomycosis is difficult due to late admission of patients to specialized departments, prolonged intoxication and the development of irreversible changes in organs and tissues. The selection of antibiotics is complicated by antibiotic resistance, the need to take into account the microflora accompanying actinomycosis, and associations of microorganisms. Difficulties also arise when performing radical surgical operations, which requires particularly careful preparation of patients for them, the use of adequate pain relief techniques and surgical tactics.
For more than 40 years, we have been using the domestic immunomodulator actinolysate in clinical practice, for the invention of which our scientists received a State Prize in 1950. This drug is a freshly prepared, stabilized filtrate of the cultural fluid of self-lysing actinomycetes and is a natural substance for the body; absence of toxicity was tested in 1124 patients. Actinolysate is highly effective and tolerant, which explains its advantages over other immune drugs. A powerful immunomodulatory effect, stimulation of phagocytosis, and an effect on reducing the intensity of inflammation have been tested in vitro, confirmed in animal experiments and in clinical practice in the treatment of more than 4 thousand patients with purulent diseases of the skin, subcutaneous tissue and internal organs.
The drug is indicated for adults and children both for the most severe chronic purulent infections, such as actinomycosis, and for milder purulent lesions of the skin, subcutaneous tissue and mucous membranes, as well as for microbial eczema, trophic ulcers, bedsores, hidradenitis, purulent-complicated wounds, urethritis and vulvovaginitis, paraproctitis, etc.
Actinolysate is prescribed 3 ml IM twice a week: there are 10-20-25 injections per course; subsequent courses are carried out at intervals of one month, according to indications.
Antibacterial therapy requires compliance with a number of general rules, including targeted action on the causative agent of the disease (actinomycetes and other bacteria). The frequency of seeding of aerobic microflora from the focus of actinomycosis is, according to our data, 85.7%. The microbial composition is dominated by staphylococci (59.8%) and Escherichia coli (16.9%); with pararectal localization, associations of several microorganisms take place. We found a higher resistance of microflora to antibiotics in actinomycosis than in acute purulent-septic diseases, which is explained by the long-term previous use of various chemotherapy drugs in these patients. Antibiotic resistance, in turn, promotes the activation of secondary microflora, including non-spore-forming anaerobic microorganisms. Through the use of actinolysate, it is possible to significantly increase the effectiveness of treatment of common purulent diseases and at the same time reduce the doses of antibiotics. This is especially important due to the increasing incidence of resistance to chemotherapy and the emergence of severe adverse reactions to them. When fungal-bacterial associations are identified, antifungal drugs are prescribed: Diflucan, Orungal, Lamisil, Nizoral, etc. Along with actinolysate, antibacterial and antifungal antibiotics, vitamin therapy, symptomatic medications, physiotherapeutic treatment with ultrasound, etc. are indicated.
In the complex of therapeutic measures for actinomycosis, surgical interventions occupy a significant place. Surgical treatment of patients with actinomycosis of the face and neck in the abscess stage involves opening and draining the lesions. In the literature there are descriptions of rare surgical interventions, for example, temporoparietal craniotomy and lobectomy with removal of an abscess in a patient with actinomycosis of the brain. For actinomycosis of the lungs and colonization of pulmonary cavities by actinomycetes, lobectomy is performed, sometimes with resection of the ribs, opening and drainage of purulent cavities, cavities and foci of decay. In the case of actinomycosis of the axillary and groin areas, which developed against the background of chronic hidradenitis suppurativa, the lesions are excised, if possible in a single block, within apparently healthy tissues. Depending on the object of the operation, the depth and area of the surgical field, surgical interventions are completed by tightly suturing the wound, autodermoplasty according to Thiersch, or open management of the postoperative wound is practiced with the application of dressings with antiseptic ointments that clean the wound and enhance regeneration; Film-forming aerosols are also used (Figure 6).
The development of actinomycosis against the background of inflammation of the epithelial-coccygeal cyst or urachus, as a rule, is accompanied by the spread of the process to the buttocks, pararectal area, and sometimes to the pelvic tissue. If it is impossible to radically remove the source of infection, they are limited to partial excision or curettage of the fistula tracts; such patients require several staged operations.
Treatment of extrasphincteric pararectal actinomycosis is carried out using the ligature method - a thick silk ligature, after excision of the lesion, is passed through the wall of the rectum above the sphincter and a pararectal incision. The ligature is tightened tonically and during subsequent dressings it is gradually tightened to cut the sphincter.
Difficulties in treating actinomycosis of the lumbar, gluteal and femoral regions with damage to the retroperitoneal tissue are due to the peculiarities of the anatomical location of the lesions, the depth of the long tortuous fistulous tracts, the tendency of patients to develop intoxication, persistent anemia and amyloidosis. After careful preoperative preparation, they resort to excision of foci of actinomycosis, complete or partial curettage of fistula tracts, opening and drainage of deep foci of abscess formation.
With the development of the actinomycotic process in the mammary gland, sectoral excision of foci of actinomycosis is performed with preliminary staining of the fistula tracts.
Patients with actinomycosis of the anterior abdominal wall are operated on after revision of the fistulas and identification of their possible connection with the omentum and adjacent intestine (Figure 7).
In the postoperative period, anti-inflammatory and immunomodulatory therapy with actinolysate is continued, blood transfusions and physical procedures are performed according to indications, and dressings are performed daily. In cases of postoperative wound healing by primary intention, the sutures are removed on the seventh or eighth day. In the first days, on wounds that are treated openly, bandages with iodoform emulsion, 1% dioxidine solution, and 1% iodopyrone ointment are applied to activate granulations. For the purpose of wound sanitation, broad-spectrum antiseptics are used. To cleanse wounds from purulent-necrotic discharge, water-soluble ointments are used: levosin, levomekol, dioxykol, as well as iruksol, panthenol, vinylsol, film- and foam-forming aerosols. To accelerate the regenerative process and epithelization, bandages with methyluracil ointment, solcoseryl, vinylin, sea buckthorn oil, etc. are applied.
In order to promptly diagnose and effectively treat actinomycosis, which is characterized by a variety of localizations and clinical manifestations, it is necessary to know the etiology and patterns of its pathogenetic development, predisposing factors, microscopic and cultural characteristics of pathogens, treatment regimens with actinolysate and chemotherapy, and surgical tactics.
S. A. Burova, Doctor of Medical Sciences. National Academy of Mycology. Center for Deep Mycoses, City Clinical Hospital No. 81
How does oral actinomycosis appear?
Most often in the body, radiant fungus is found in gum pockets, carious cavities, dental calculus, tonsil lacunae, damaged or inflamed tissues of the oral cavity, nose, salivary glands, and gastric mucosa.
The fungus can also enter the body from the outside, from the environment. Microorganisms can stay in the body for a long time without causing any harm until the mucous membrane is damaged. Actinomycetes spread inside the human body mainly through the blood (hematogenously), and occasionally they talk about the possibility of entering various organs through the lymph (lymphogenously). In order for the disease to develop, it is necessary to repeatedly enter the body with radiant fungi. Most often, the patient himself becomes infected with the fungus from his own body (autoinfection).
Before the first symptoms of the disease appear, it usually takes 1 to 3 weeks after actinomycetes enter the body. In general, the incubation period can vary from a couple of weeks to 2-3 years.
Radiant mushrooms are also common in nature (in soil, hay, straw or on plants). People of mature age, schoolchildren and preschoolers suffer from actinomycosis more often. The cervicofacial region and lower jaw are most often affected by infection.
The impetus for infection with actinomycosis can be injections, injuries or surgical operations. For actinomycosis to develop, it is enough to injure the mucous membrane with a fish bone, damage it with a fragment of a carious tooth, bite the cheek, or have gums damaged by inflammation.
Diagnosis of actinomycosis
The diagnosis of actinomycosis is made based on the following studies:
- Microbiological examination of secretions
- Skin allergy test with actinolysate
- X-ray examination
Microbiological examination is the simplest method for diagnosing actinomycosis. Cytological examination of stained smears allows the identification of actinomycetes and secondary infection. If this method does not provide a comprehensive answer, then it is necessary to isolate actinomycete cultures by sowing.
A skin allergy test is performed according to Asin : 0.3 ml of actinolysate is injected into the thickness of the skin on the surface of the forearm. At a distance of 10 cm from the actinolysate, 0.3 ml of meat-peptone broth is introduced. After an hour, blisters appear, which soon (1-2 hours) disappear and erythema appears in their place. In healthy people, the erythema disappears within 12 hours, but if a person is sick, the erythema will disappear only after 36-48 hours.
X-ray examination plays an important role in the diagnosis of primary and secondary bone lesions by actinomycosis. And for the diagnosis of actinomycosis of the salivary glands, sialography is widely used.
Symptoms
The cervical-maxillofacial form of the disease (genitourinary, skin, abdominal, osteoarticular, thoracic and other forms are also found) occurs most often, in almost 80% of cases of actinomycosis.
At the beginning of infection or self-infection, the patient’s well-being does not suffer in any way. The cervical-maxillofacial form occurs in several forms with damage:
- skin (cutaneous form);
- mucous (mucous form);
- subcutaneous tissue and muscles (subcutaneous muscle form);
- jaw bones (jaw shape).
The disease has a very long course and can last 10-20 years. Gradually, the pathological process can spread throughout the face, reaching the lips, tongue, larynx, involving the eye sockets and penetrating the neck area.
The muscular form most often affects the masticatory muscles.
Most often, actinomycosis of the oral cavity affects the tongue, salivary glands or tonsils. Actinomycosis of the upper jaw is less common.
Actinomycosis of the tongue
Actinomycosis of the tongue usually develops with chronic injuries to this organ with poorly fitting dentures, sharp broken edges of teeth, damage to the lingual tissues by sharp bones, after tongue piercing, etc. The clinical picture of the disease depends on the location of the source of infection. If the tip of the tongue or its back is affected, then these areas will not have any external changes for a long time and will not hurt. However, after some time, the actinomycosis node becomes fused with the mucous membrane of the tongue or becomes abscessed, resulting in the formation of a fistula in the node.
Actinomycosis of the tonsils
Actinomycosis of the tonsils is less common than other forms. With this form, the tonsils are enlarged and compacted, resembling cartilage in density. Subsequently, the pathological process spreads to neighboring tissues. The main symptom of this form of the disease is the feeling of a foreign body in the pharynx.
Actinomycosis of the salivary glands
Actinomycosis of the salivary glands can be primary or secondary. More often, the radiant fungus enters the salivary gland through the duct. There are several forms of this type of actinomycosis:
- exudative limited and diffuse disease;
- limited productive and diffuse disease;
- lesions of the deep lymph nodes in the area of the ear gland.
Actinomycosis of the maxillary sinus
Actinomycosis of the maxillary sinus is rare. In this form, the infection enters the jaw from the affected tooth (odontogenic pathway) or from the nose (rhinogenic pathway). Manifestations of actinomycosis of the upper jaw resemble sinusitis: nasal breathing is impaired, and purulent discharge may come out of the nose. During exacerbation, swelling of the zygomatic, buccal and infraorbital areas is noticeable.
What manifestations should alert the patient and force him to see a doctor for actinomycosis?
At the onset of the disease, it is difficult to detect due to the normal temperature and good health of the patient.
Although the mucous membrane is already damaged and lesions in the form of nodes begin to form in the tissues, the pathological process can proceed deeply and not be noticeable externally.
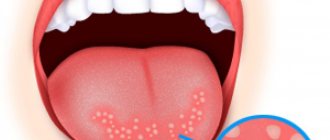
If actinomycosis affects the oral mucosa, the patient will experience symptoms such as:
- swelling on the oral mucosa;
- inflammation and pain in the mouth;
- formation of fistulas in the oral cavity with the release of purulent fluid.
The local course of the disease and the absence of general signs of intoxication are characteristic of all forms of actinomycosis.
Actinomycomas or granuloma nodules can be found in tissues or mucosa. And only at the stage of disintegration of these nodes, pus is released from them and intoxication processes occur in the body (poisoning with tissue decay products).
Symptoms appear in the patient only at the stage of node disintegration. In this case, pus is released from fistulas (channels in the node).
At the stage of nodular decay, the patient is concerned about manifestations in the form of:
- headache;
- temperature (usually 38-38.5 degrees);
- general weakness;
- poor appetite.
When the nodes are located on the lower jaw, there may be spasms of the mouth in the form of convulsions (trismus), which interfere with eating.
Clinical picture
The disease, as a rule, has an acute onset and resembles a purulent-inflammatory lesion of the soft tissues of the face (abscess, phlegmon and periostitis). The pathological process is accompanied by subfebrile body temperature (37°C), and in some patients hyperthermia is not observed. The patient's main complaints during this period are reduced to the occurrence of local pain at the site of fungal penetration.
After 1-2 weeks, the disease transforms into chronic actinomycosis, which is accompanied by periodic exacerbations and relapses. Local manifestations of infection consist in the formation of a limited focus of infiltration with areas of suppuration. After opening the actinomycosis lesion, it actively regresses.
Actinomycosis of the buccal region
The main symptoms of the disease include:
- increase in body temperature, the magnitude of which depends on the level of general immunity;
- limited mobility of the lower jaw;
- inflammatory swelling of the soft tissues of the maxillofacial area;
- the subcutaneous muscular form of actinomycosis is characterized by severe pain, impaired chewing and pain when swallowing food;
- when bone tissue is involved in the pathological process, the patient experiences numbness of the skin in the chin area due to compression of the inferior alveolar nerve;
After 3-4 weeks, actinomycosis provokes an inflammatory reaction from the lymphatic system in the form of enlargement and swelling of regional lymph nodes.
Main forms of actinomycosis
The variety of symptoms of fungal infection is due to the localization and spread of actinomycosis.
In dental practice, the following forms of the disease are distinguished:
- Skin appearance. This type is extremely rare (1.9% of clinical cases). A sign of cutaneous actinomycosis can be considered the formation of granuloma in the epidermis or subcutaneous layer, which gradually causes the replacement of skin tissue with connective tissue structures. The introduction of a fungal infection into the skin occurs when it is externally damaged or in an odontogenic way.
In such cases, single or multiple ulcers form on the patient’s skin, after opening which purulent fluid flows out with individual grains of radiant fungus. After some time, such areas become covered with dense tubercles.
- Subcutaneous view. A distinctive feature of this lesion is fungal infiltration of the subcutaneous tissue in the area of the causative tooth. The actinomycosis focus is localized in the area of the chin or cheeks.
- Submucosal appearance. The disease develops as a result of injury to the oral mucosa by foreign bodies, sharp edges of teeth, or the spread of odontogenic infection. Patients complain of slight pain in the purulent lesion, which intensifies when talking and eating. The mucous layer acquires a grayish tint and gradually thickens. All these pathological changes occur against the background of a normal temperature level.
- Slimy appearance . In this case, the inflammatory-purulent focus has a round shape and is located in the superficial layers of the mucous membrane of the oral cavity and lips. After opening the abscess, a bloody-purulent surface is exposed. The disease is characterized by a sluggish and painless course.
In the later stages, the presence of a large dense focus of suppuration with areas of softening in the central part is considered typical for actinomycosis. The skin in this area is bright red. Purulent fluid leaks from the wound surfaces.
Actinomycosis of the cervical region
Features of actinomycosis in children
In children, the disease occurs much less frequently than in adults. In this case, the main sources of fungal infection are carious teeth and inflamed tonsils. In such cases, the pathological process tends to quickly spread to nearby soft tissues and lymph nodes.
Unlike actinomatous lesions in adults, in children the disease ends with sealing of the tissues of the maxillofacial area. Actinomycosis in pediatric patients is often accompanied by a pronounced periosteal reaction in the form of pathological growth of bone tissue of the upper or lower jaw.
Forms of actinomycosis
With actinomycosis of the oral cavity, infectious foci develop in the tissues of the oral mucosa.
Actinomycosis of the oral cavity can also occur in three forms:
- Gummy-nodular, with characteristic red or brown infiltrates. In this case, the skin in the affected areas softens, fistulas form on it, from which purulent fluid with inclusions is released.
- Tuberous-pustular, in which deeper ulcers are formed, combined with the formation of pustules and fistulous canals. This form is characterized by the appearance of purulent crusts on the skin.
- Ulcerative, in which there are skin defects of varying depths. Skin ulcers subsequently lead to tissue scarring and cicatricial atrophy.
What happens if actinomycosis is not treated?
Inside the tumor, ulcers form, covered with purple, increasingly thinning skin. They gradually approach the surface and then open up. A purulent fluid is released containing fat cells, fibrin and, above all, grains with fungal drusen. If a secondary infection occurs, phlegmon and large abscesses may develop.
Actinomycosis does not spread through the lymphatic tract, but the ulcers can open into the vessels, due to which the fungus penetrates the blood and is carried into all tissues and organs. This picture ends in death. Death occurs from exhaustion or amyloid degeneration, due to the absorption of decay products, and not from the action of a specific poison.
Actinomycosis of the oral cavity in children
In pediatrics, actinomycosis is not so rare and usually occurs more often in children with carious teeth, frequent inflammation of the tonsils, or with the habit of putting or chewing various spikelets and stems of plants (especially barley, rye, oats, sorrel) in their mouths.
After damage or microtrauma to the mucous membrane, the fungus enters the tissue and causes a red swelling to appear in the mouth, which grows slowly. In some cases, actinomycosis may manifest itself in the form of acute phlegmon (spread inflammation). In this case, the swelling suppurates, but no outflow of pus occurs.
Phlegmon occurs in a child with local pain and spastic clenching of the jaws due to tissue swelling (if the neck and chin area become inflamed), which prevents the baby from opening his mouth.
After suppuration, the purulent formation can open on its own and form fistulas. With actinomycosis of the tongue, a visible infiltrate (swelling) usually forms on its front part.
Clinical manifestations of the disease in children
Just like in adults, actinomycosis in children begins in the form of local (limited) inflammation, which does not affect the general well-being of the patient. The course of the disease becomes chronic, with the temperature being low or high.
If a child's disease is not treated, it can become generalized (with multiple lesions) and lead the child to complete exhaustion (cachexia). This is due to constant intoxication, poor appetite and difficulty chewing food.
What is actinomycosis
The content of the article
Actinomycosis is a subacute chronic bacterial infection caused by filamentous, gram-positive, non-acidic, anaerobic and microaerophilic bacteria. The disease is characterized by purulent and granulomatous inflammation and the formation of multiple abscesses and sinus tracts that may secrete sulfur granules.
The most common clinical forms of actinomycosis are cervicofacial (jaw), thoracic and abdominal. In women, pelvic actinomycosis is possible.
Diagnostics
Actinomycosis has similar manifestations with many infectious and inflammatory processes in the skin (phlegmon, abscess) or bone (osteomyelitis, periostitis), some infectious diseases (syphilis, tuberculosis) and tumor diseases.
In the diagnosis of actinomycosis, in addition to examining and collecting anamnesis from the patient, the use of diagnostic research methods is also used in the form of:
- blood and urine tests (general, biochemical) to determine the nature of the existing infectious inflammation;
- microbiological, to determine the colony of actinomycetes in the infiltrate;
- immunological, most often in the form of a skin allergic reaction in the form of subcutaneous administration of actinolysate;
- pathohistological, with examination of granulation tissue under a microscope.
- X-ray (when the process moves to the jaw bones) with determination of the bone cavity;
- biopsy with examination of granuloma tissue to exclude oncology.
Diagnosis of radiation fungus lesions
Actinomycosis is usually a polymicrobial infection with isolates numbering up to 5-10 species of bacteria. Therefore, detection of this infection in humans may require testing for associated bacteria that are involved in maintaining the disease by producing a toxin or enzymes or by inhibiting the host's defenses.
To recognize actinomycosis, they are guided by the clinical picture and, above all, by the presence of drusen-containing granules in fresh pus, sputum and feces. It is possible to mix with other types of infectious granulomas, namely tuberculosis, syphilis, or true tumors.
Associated bacteria act as copathogens that increase the relatively low invasiveness of actinomycetes. In particular, they are responsible for the early manifestations of actinomycosis and treatment failure.
Treatment
Treatment of actinomycosis of the jaw and oral cavity is always carried out with the simultaneous use of general and local therapeutic measures.
The main types of therapeutic measures for actinomycosis are the following methods:
- Surgical treatment. This method includes removal of carious teeth, tonsils, opening of foci of actinomycosis, curettage of pathology inside the bone, and removal of affected lymph nodes. Actinomycosis lesions and purulent wounds are also surgically treated.
- Anti-inflammatory treatment. Includes antibiotic therapy in the form of intravenous Penicillin for up to 6 weeks and a transition to intramuscular administration of it or Amoxicillin for 6-12 months. Amoxiclav, Doxycycline, Phenoxymethyl, and Erythromycin are often used orally. This also includes the use of antifungal agents: Nystatin, Levorin, Miconazole, Ketoconazole, Decamine, potassium iodide preparations.
- Methods for developing specific immunity. To do this, patients undergo intradermal administration of actinolysate or actinomycetic polyvalent vaccine (course of 20-25 injections) or long-term course use of Ftivazid (from 3 to 8 months).
- Increases general immunity. Methods of vitamin therapy (complexes of vitamins and microelements), the use of adaptogens (Dibazol, ginseng, Eleutherococcus, pantocrine, Manchurian aralia, etc.), autohemotherapy, intravenous administration of blood or blood substitutes are used.
- Treatment by staying in a pressure chamber in the amount of 10-15 procedures per course.
- X-ray therapy in the form of the use of X-rays according to an individually selected scheme.
- Physiotherapy using ultrasound, electrophoresis (with lidase, dimexide, calcium chloride), laser therapy, iontophoresis with hydrocortisone, ultraviolet radiation.
Diagnosis and treatment principles
Diagnosis of actinomycosis is not associated with any difficulties in cases of a detailed typical clinical picture. The initial stages of the disease are much more difficult to diagnose. A certain importance in diagnosis is attached to an intradermal test using actinolysate, however, only positive and strongly positive reactions are taken into account, since a weakly positive test can also occur in other diseases, and a negative one is not a reason to exclude the disease, since it can also be such with suppressed immunity. In 80% of cases of actinomycosis, the reaction of complement binding with actinolysate is positive. The most reliable detection of actinomycetes in pus secreted from fistulas, in tissue biopsies, in drusen, including by inoculating materials on a nutrient medium (cultural diagnostics), X-ray, histological (microscopic) studies.
Differential diagnosis
It is carried out mainly with lupus, colliquative tuberculosis of the skin (scrofuloderma), with abscesses caused by ordinary purulent infection, with benign and malignant neoplasms.
Therapy
Due to the characteristics of the causative agent of actinomycosis, the mechanisms of its development and the variety of clinical manifestations, treatment of actinomycosis should be comprehensive, including:
- the use of anti-inflammatory drugs, including antibiotics, taking into account the sensitivity of the accompanying microflora to them;
- carrying out immunomodulatory therapy using actinolysate;
- use of restorative drugs;
- physiotherapeutic effects (iodide phonophoresis, UHF and UV radiation, etc.).
If necessary, surgical treatment is carried out, the meaning of which is to excise the foci, complete or partial curettage of the fistula tracts, etc. Curing actinomycosis does not exclude its relapses.
Watch a video about Actinomycosis:
Complications and prognosis
The prognosis for this disease is quite serious. It is important to identify and treat actinomycosis as early as possible.
Some forms of actinomycosis of internal organs can be fatal in the absence of specific therapy. For example, mortality in abdominal and pulmonary forms of this disease can reach up to 50%.
The maxillofacial form of actinomycosis is considered the mildest and is more treatable than other forms. However, even after successful treatment, the patient must be registered at the dispensary for 6 to 12 months.
A prolonged course of the disease in the maxillofacial area can lead to dangerous complications in the form of metastasis to internal organs: the meninges, the lung area, and the gastrointestinal tract. In some cases, actinomycosis can lead to complications in internal organs in the form of amyloidosis (a disease leading to atrophic changes and hardening of internal organs).
The most serious complication of actinomycosis is the occurrence of actinomycosis sepsis.
The prognosis for timely treatment of actinomycosis is generally favorable if therapy is started in a timely manner and carried out correctly. However, this disease can have a long course (as with tuberculosis), leading to repeated relapses.
Actinomycosis reviews
Katerina, 42 years old, Khabarovsk region.
Actinomycosis is a serious and unpleasant skin disease that can only be experienced. It just so happened that I ran into him last year. First, a small 3-5 mm red spot appeared on the right cheek. I didn’t pay attention, thinking about a pimple, etc. But after a week the spot began to swell and grow. I ran to the hospital. The doctor told me to get tested. Cytological examination revealed inflammation. The diagnosis was “actinomycosis of the facial area, purulent masses.”
With this terrible diagnosis for me, I went to the doctors, but to my surprise, in our rather large hospital, no one had heard of such a disease. I had to go to the regional center and see specialists at a private clinic. The doctors did several tests (blood, scraping, mushrooms), prescribed antibiotic injections - Ceftriaxone solution (India) and drugs to boost immunity.
In short, I was treated for four months. Doctors say that I was lucky, because I immediately turned to specialists and did not delay. Complications of actinomycosis can bring the patient to the operating table, so do not delay going to the doctor. Thank you for your attention.
Tatyana Aleksandrovna Pukhova
Dermatologist , 14 years of experience.
Generalist specialist. Engaged in the diagnosis and treatment of diseases of the skin, nails, scalp, as well as sexually transmitted diseases.
Education: 2006 Diploma in General Medicine, Perm State Medical University
Advanced training courses: 2011 “Pillings of superficial-medium impact” 2013 “Plasmolifting in cosmetology and trichology” 2014 “Dermatovenereology”, South Ural State Medical University