The digestive system begins with the oral cavity. Here mechanical processing of incoming food is carried out.
The surface of the mouth is covered with a mucous membrane, designed to protect it from any irritants.
The structure and design of the oral mucosa is very complex and has its own characteristic features that distinguish it from other organs of the human body.
All these unique features allow the shell to perform a large number of functions.
Histology of the mucous membrane
The oral cavity is enveloped in a membrane.
It covers the inside of the cheeks, lips, alveolar processes, palate, tongue and floor. It is constantly moisturized thanks to the work of the salivary glands and has characteristic properties in its structure and implements functional tasks. The most important functional actions:
- Protection . It protects the coating from mechanical stress, from harmful bacteria and microbes that come from food.
- Improved digestion . Salivary glands produce saliva, which helps digest food.
- Feel . It helps to recognize taste, temperature, swallow food and respond to external stimuli.
- Regulate heat . Breathing through your mouth helps you warm your hands or regulate your body temperature.
- Maintaining immunity . The mouth contains cells that affect the overall immunity of the body.
- Suction . Some trace elements and medications can be absorbed through the oral cavity.
The mouth covering can perform all these functions due to its unique structure. The surface structure is quite heterogeneous and complex. In some parts it can move and is flexible, in others it is motionless.
The following layers of the oral mucosa are distinguished:
- epithelial layer;
- directly mucous layer;
- submucosal layer.
The entire shell is enveloped in a flat epithelial layer, which has many layers. In different parts of the cavity it has a different structure. In areas of the soft palate, lips, cheeks and floor, it consists of a basal layer and a layer with spines and is not capable of keratinization. Areas of the hard palate and gums are covered with granular and horny layers, because have the ability to keratinize.
The process of hardening and exfoliation of particles occurs due to the fact that mechanical action is applied to individual areas. This is the result of a response to irritation. Almost half of the entire area of the mouth is susceptible to keratinization.
The thickness of the epithelium varies in different areas. Places where the impact of external irritants is minimal - the bottom of the mouth, the lower part of the tongue and lips - the cover is very thin. In other areas it is much thicker. As a person ages, the thickness of the layer changes. In childhood it is very thin, then gradually thickens and thins again in old age.
After the epithelial layer comes the mucous layer. Its basis is connective tissue. With the help of papillary-shaped elevations, it passes into the epithelial layer. Each papilla is equipped with many nerve fibers and blood vessels. Thanks to this connection of the two layers, nutrients are exchanged between them and they are firmly united.
The mucous layer contains glands of salivary secretion, sebaceous secretion and lymph nodules. This layer smoothly flows into the submucosal layer. It is transformed into loose connective tissue containing the smallest glands of salivary secretion and vessels of the hematopoietic system.
The submucosa contains a type of fat cells that are responsible for the ability to move. This layer is characteristic of areas not subject to keratinization - the bottom of the mouth, cheeks and lips.
Oral mucosa
The oral mucosa is part of the mucous membrane of the entire gastrointestinal tract. Each section of the digestive tract has this characteristic lining. Its name already pinpoints its location. In the mouth, this type of mucous membrane is formed by taste buds and salivary glands.
The mucous membrane of the pharynx performs such functions as:
- protective functions of the oral cavity, which consist in preventing the passage of most microorganisms through the epithelium and ensuring the “passage” of harmful substances due to the saliva formed in the oral cavity and the lysozyme contained in it,
- ability to distinguish between temperatures (from very hot to icy),
- the ability to feel pain due to the presence of sensory receptors,
- ability to feel pressure
- the ability to distinguish different tastes thanks to taste buds,
- absorption of many substances, known as the resorptive function of the oral mucosa,
- renewal of the epithelium due to its specific structure.
The oral mucosa is covered with flat stratified epithelium, keratinized or non-keratinized. This type of epithelium provides a balance between the formation of new cells and the removal of old ones. This is why medicine places so much emphasis on the ability to renew the oral mucosa.
Poor oral hygiene or irritants (such as physical, thermal or mechanical) can cause oral inflammation. This causes inflammation, ulceration, and viral and fungal infections. Very often, such unfavorable changes occur during puberty, pregnancy or menopause.
Inflammatory changes in the mucous membrane also occur with certain infectious diseases, vitamin deficiencies or ailments associated with gastrointestinal diseases. Many factors negatively affect the oral mucosa. One of the most common causes is aphthous stomatitis, the presence of bacteria, celiac disease (that is, gluten intolerance), allergies to certain foods, or serious diseases such as cancer.
But very often the causes of inflammation of the mucous membrane are quite ordinary, for example, biting the cheek, excessive brushing of teeth, or eating too sour or spicy foods.
About
Innervation of the oral cavity
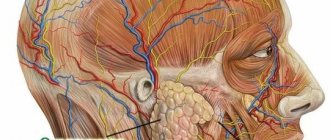
The inner lining of the mouth is penetrated by a huge number of nerve endings and fibers. Thanks to them, nerve impulses are transmitted to the central parts of the brain. The sensory function of the mouth allows a person to sense the taste, shape, and temperature of external stimuli.
All the fibers along which the impulses travel are connected to the main nerves of the oral surface:
- trigeminal nerve;
- facial nerve;
- glossopharyngeal nerve;
- nervus vagus.
The structure and direction of nerve fibers is similar to the trunks of blood vessels. The fibers are located in the mucous layer and are intricately intertwined with each other, forming nerve endings.
Some of them extend to the papillary processes and connect to the epithelial layer, some of them unite with the cells above and extend to the upper edge. Such a complex network of fibers and nerve endings covers the entire coating structure in all its layers.
A complex system of nerve endings allows the oral cavity to have very strong sensitivity and respond to the slightest irritation. It is a unique organ of the human body through which it perceives the world around it.
Blood supply and lymphatic drainage
The membrane is equipped with an abundance of blood vessels. They look like arteries that are located in the submucosal layer and run parallel to the mucous layer. The arteries branch with branches perpendicular to the mucous layer. Most of the processes are present in the layer of papillae and are very densely intertwined near the epithelium.
Capillaries differ in their structure depending on their location. The capillaries of the bottom of the mucous membrane and gums have fenestrated epithelium, and on the cheeks the lining is continuous. The vessels located along the venous bed are similar to the main arteries.
The cavity is also equipped with lymph drainage. The vessels of the lymphatic system begin with small capillaries with a wide lumen. They are located at the papillae connecting the mucous and epithelial layers. Gradually, the lymph capillaries unite into vessels and are directed similarly to blood vessels. The junction of all vessels is the lymph nodes. All lymph from the membrane is transferred to the submandibular or cervical lymph node.
The mouth has a highly developed blood supply system. This allows it to quickly regenerate and renew keratinized particles. With good blood flow, the oral lining can perform functions such as protection, absorption and immune support.
Structure of the oral cavity
Let us consider in detail each component of the oral cavity, its structure, purpose and functions.
Lip
The lips are circular muscles. Their outer side is covered with skin, and the inner side is covered with mucous membrane. Between the two sides there is a border with a transitional structure. It lacks sweat glands and hair, but does have salivary glands. This border is a characteristic feature of humans, unlike other animals.
The submucosal layer of the mucous membrane of the lips is tightly connected to muscle fibers. Thanks to this, the lips are very smooth and wrinkles do not form on them. The mucous membrane of the lips contains a large number of salivary glands. It mixes tightly with the epithelial layer through many blood capillaries, which are located near the surface and are practically invisible through it. This explains the red color of the lips.
The labial mucosa is similar to the oral cavity. This part is not adapted to keratinization. There are practically no sebaceous glands here and salivary glands predominate. They have a complex structure in the form of tubes, and secrete a more mucous secretion.
In small children, the lips are relatively thicker, but at the same time they have a thinner epithelial cover. The main features and structure of the lips develop gradually, and this process ends at about 16 years of age. As the body grows, changes also appear in the structure of the lips. The papillae between the layers are smoothed out, the collagen fibers become thinner and a lot of adipose tissue is formed in the submucosal layer.
The lips are equipped with many nerve endings. Thanks to this, the lips are very sensitive. There are frenulums on the upper and lower sides of the lips. These frenulums include collagen and elastic fibers. When attached closely to the gums, frenulums can affect the mobility of teeth and contribute to their displacement.
Cheek
The buccal covering is similar in structure to the oral membrane and serves as its continuation. It contains a thick epithelial layer that is not capable of keratinization. The mucous membrane is formed by dense connective tissue with elastic fibers. This layer gradually flows into the submucosal layer and is tightly attached to the muscle fibers on the cheeks.
The presence of elastic fibers in its composition, as well as a strong connection with muscle fibers, allows the surface of the cheeks to have the ability to be smooth and elastic. The submucosal layer contains adipose tissue and small salivary glands. Fatty deposits and glands can form clumps that can be mistaken for a tumor.
Upon examination, the covering on the cheeks and lips has a fairly smooth surface. But upon closer examination, several characteristic properties can be seen. On the side in the area of the second molar on top there is a papilla with an opening through which saliva flows from the parotid salivary gland. In the center of the upper and lower lips there are folds or frenulums that serve as a border for the right and left halves of the mouth.
At the level where the teeth meet, the buccal mucosa is slightly different from other areas. There are no salivary glands here, but sebaceous glands are present and the epithelial cover is capable of keratinization. In infants after birth, this part is covered with villi, similar to the villi on the red border.
The cheeks are well supplied with blood. Blood flow occurs due to small salivary glands and cells. The mucous membrane of the cheeks contains a network of small blood vessels that are densely intertwined and supply blood to the cheeks.
Solid sky
The surface of the hard palate in some areas does not have the ability to move. This is due to the fact that in these sections it is tightly fused with the palatine bones. The submucosal layer is also absent in these places.
Among the fixed areas are:
- area adjacent to the tooth or marginal zone;
- section in the area of the suture in the palate, where the mucosa is fused with the periosteum.
In other areas of the hard palate there is a submucosal layer. In areas in front there is adipose tissue, and in distant areas there are a large number of small salivary glands.
The entire area of the hard palate is divided into 4 sections:
- fatty;
- glandular;
- seam area;
- edge zone.
The mucous layer is expressed by connective tissue with the presence of collagen fibers. It is entirely covered with an epithelial layer with many layers and the ability to harden and exfoliate scales. The connection between the mucous and epithelial layers occurs with the help of high papillae with sharp tips.
The area of the hard palate has several irregularities. Near the incisors in front, there is a papilla on the suture at the anterior end. In this area, blood vessels and nerve fibers pass through the bone. There are also transverse stripes in the front part of the seam. They are quite clearly visible in small children, but as they grow older they become smooth and barely noticeable.
The blood flow to the palate passes through the arteries. Through the papilla of the anterior incisors, blood flows to small branches in the mucosa, and then scatters into capillaries in the submucosal layer. Then the capillaries again carry the blood to the veins.
The area of the hard palate in front is washed with blood from the incisive artery, similarly, blood leaves through the incisive vein and the vein of the nasal cavity. There are a lot of lymph vessels here, through which lymph drainage occurs. The hard palate is also rich in nerve endings. The main number of nerve fibers are present in the mucous membranes of the anterior section.
Soft sky
The soft palate has the appearance of a fibrous plate on which striated muscles and mucous membrane are attached. It is covered with a shell on all sides. There is a small process on it - a tongue.
The surface of the palate and uvula below is covered with a flat epithelial layer, which is not capable of keratinization. The mucous layer is formed by connective tissue. At the transition between the mucous and submucosal layers there is a large number of elastic fibers. The submucosal covering of the soft palate contains the ends of many salivary secretion glands, their apices pass through the open part of the mucosa.
The distal portion of the soft palate extends toward the nasopharynx and is covered by a multirow epithelial layer that is exclusive to the respiratory tract. In small children, multirow epithelium is also present on the distant part of the uvula. But with age, it is replaced by a multilayered one, and in an adult, the uvula is covered on all sides with a regular epithelial layer.
It is well supplied with blood through many vessels of the circulatory system. The capillaries are located near the edge of the mucosa and cause the red color. Lymph drainage in the soft palate is carried out thanks to lymph nodes.
Gum
The gum is the area of the oral membrane that covers the alveolar processes of the jaws and touches the teeth. It consists of a multilayered epithelial cover that can become keratinized. The process of keratinization noticeably occurs on the vestibular part of the gum; on the oral side, parakeratosis very often occurs.
The mucous layer of the gums is very similar to the dermis of the skin. It consists of two layers:
- a layer of papillae made of loose connective tissue;
- a mesh-like layer consisting of dense tissue and an abundance of collagen fibers.
The papillae have a complex structure, different shapes and sizes. In some parts they form branches. It is through them that the main network of vessels of the circulatory system and the endings of the nervous system passes.
The submucosal layer and salivary glands are practically absent. The mucous membrane grows into the periosteum of the alveolar jaw processes. In the area of the dental neck, fibers of the circular dental ligament grow into the mucous layer, and as a result, the gums are able to adhere closely to the teeth.
The area of the gum that is fused with the periosteum is called the attached gingiva. The area of gum that lies freely near the tooth and is separated from it by a section in the form of a gap is called free gum.
The attached and free gums are separated by a groove. It runs along the edge of the gum at a distance of 0.5-1.5 mm and characterizes the gingival crevice. The area of gum between the teeth is called the interdental papilla. They are covered with stratified epithelium, but keratinization often turns into parakeratosis.
From the alveolar processes, the gums smoothly flow into the membrane covering the jaws. At the transition there is an uneven, loose epithelial cover. The surface of the jaws further connects with the periosteum and flows into the folds of the lips or cheeks, the marginal zone of the hard palate or the floor of the mouth.
The gum gap is the distance between the tooth and the free edge of the gum. In a healthy state, the bottom of this gap reaches the level of the cervical enamel or cementoenamel border. The epithelium in the gingival crevice is firmly attached to the tooth. This site of attachment is called the epithelial attachment.
This attachment plays a huge role in protecting the tissues around the tooth from various infections and environmental influences. As a result of the destruction of the epithelium of the gingival crevice, the connective tissue is exposed, and the gap widens into a pocket. The epithelium begins to grow along the tooth root and periodontal fibers are destroyed. The consequence of this is loosening and loss of teeth.
Language
The tongue is an organ made of muscles. It is surrounded by mucous membrane, which in some parts fuses with the muscles.
On the back above and on the surfaces on the sides, the submucosal covering is practically absent. It is in these parts that fusion with the muscles of the tongue occurs. The mucous membrane does not move here and does not form folds.
On the upper part of the tongue, stratified epithelium is present and characteristic projections called papillae are formed. Their epithelium contains taste buds. On the lower part, the stratified epithelium is smooth, does not undergo the process of keratinization, and has a characteristic submucosa.
The tongue papillae are divided into 4 types:
- in the form of threads;
- in the form of mushrooms;
- in the form of leaves;
- surrounded by a groove.
The filiform papillae are the most numerous. They are present on the entire dorsum of the tongue. They are formed from protrusions of loose tissue of the mucous membrane. In addition, the growths also entail a number of secondary projections, reminiscent of thin fibers. They are equipped with several peaks.
The epithelium on the papillae can become keratinized. Keratinized scales are characterized by a white color. The process of keratinization proceeds faster in the event of an increase in a person’s body temperature and disturbances in the digestive process.
The mushroom-shaped protrusions were named by the owl for their characteristic shape with a long base and a wide apex. They envelop the epithelium, which does not keratinize. Blood vessels pass through them very close to the surface. Therefore, the mushroom-shaped papillae, when viewed enlarged, look like red dots. They also contain taste buds.
Leaf-shaped - are parallel folds located on the sides of the tongue and are separated by narrow grooves. Usually their number reaches 8 pieces with a length of up to 5 mm.
Such nipples are clearly visible in small children and some animals. The leaf-like projections are covered with epithelium and contain many taste buds. These bulbs are oval in shape and consist of epithelial cells tightly connected to each other.
Main cells of taste buds:
- sensoroepithelial;
- supportive;
- basal;
- peripheral.
Microvilli extend from the sensoroepithelial cells and flow into the taste canal. This channel is presented on the surface of the epithelium in the form of a taste pore. Between the villi there is a chemical substance that reacts to chemical compounds and affects nerve impulses. For each taste bulb there are more than fifty nerve fibers. On the part of the tongue in front there are bulbs that recognize sweet taste, on the back - bitter taste.
The last type of papillae is grooved. They are located on the border between the main part of the language and its root. Their distinctive feature is that they are not visible on the surface of the tongue, but are hidden in its depths.
All protrusions are surrounded by mucous membrane and separated from it by a deep groove. This groove is where the protein glands drain from the muscle tissue at the base of the papillae. The epithelium around these projections contains many taste bulbs.
The salivary glands are located in the tongue:
- mixed type in the anterior section;
- mucous secretion glands at the root of the tongue;
- protein secretion glands on the border between the main part and the root of the tongue.
Blood flow in the tongue is provided by the lingual artery. They branch into a dense network of capillaries. Venous vessels run on the lower part of the tongue. The lymph flow is well developed. It passes through the vessels through the lower surface of the tongue.
The lingual tonsil is a collection of nodules in the lymphatic system. It is included, together with other tonsils, in the lymphoepithelial ring, which protects the entire body. The tonsil is covered with non-keratinizing epithelium, which forms crypts or depressions. At the bottom of these depressions there are ducts of the lingual glands of salivary secretion.
Histology and physiology of the oral mucosa
HISTOLOGY AND PHYSIOLOGY OF THE ORAL MUCOSA
STRUCTURE OF THE ORAL MUCOSA
The mucous membrane of the oral cavity, unlike other mucous membranes of the human body, has a number of features. It is resistant to physical, thermal and chemical irritants, as well as infection; the regenerative ability of the oral mucosa is increased. These properties are to a certain extent determined by its structure. Research conducted by L. I. Falin and V. V. Gemonov made a significant contribution to the study of issues of morphofunctional characteristics of the oral mucosa.
Throughout its entire length, the oral mucosa is lined with stratified squamous epithelium, consisting of several layers of cells. The basal layer is the deepest and consists of cylindrical or cubic cells. Above is the spinous layer, consisting of several rows of polygonal cells with lighter cytoplasm and pronounced intercellular connections. Closer to the surface, the spiny cells flatten, turning into flat ones. During physiological desquamation of the epithelium, flat cells are mixed with saliva.
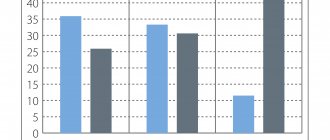
Regeneration of the epithelium occurs due to the division of cells in the deep layers. The epithelium of the mucous membrane of the cheeks, lips, soft palate, transitional folds, vestibule of the oral cavity, as well as the floor of the mouth and the lower surface of the tongue does not keratinize. A feature of the epithelial cells of the human oral mucosa is their large size, which is most noticeable in the mucous membrane of the cheeks and lips. They have a vesicular appearance and resemble the epidermal cells of the embryo in the early stages of intrauterine development. The thickness of the epithelium in different areas is not the same. The epithelium is thickest on the lips and cheeks; thin epithelium lines the lower surface of the tongue. The epithelium of the mucous membrane of the hard palate and gums exhibits clearly defined keratinization. On top of the layer of spinous cells there is a granular layer, consisting of elongated cells containing keratohyalin grains in the protoplasm. The surface layer of the epithelium of the hard palate is formed by several rows of completely keratinized and nucleated cells. In the keratinizing layer of the gums, cells retain nuclei. According to V.V. Gemonov, keratinization is found on 60% of the gum surface, and phenomena similar to parakeratosis are found on 40%; the cells of the stratum corneum retain their nuclei and are not completely keratinized. The multilayered squamous epithelium of the red border of the lips becomes keratinized, wide capillary loops of blood vessels come close to the surface and are visible through the epithelium. Keratinization of the epithelium of the red border is accompanied by the formation of elleidin, an intermediate product of the conversion of keratohyalin to keratin. Elleidin is contained in the stratum lucidum, an intensely stained layer at the border of the stratum corneum and granular layer; the contours of individual cells are not distinguishable in it. The process of keratinization of the epithelium is protective in nature and is observed in those areas that experience heavy loads when chewing. It was found that the number of leukocytes in the underlying connective tissue is negligible where the stratum corneum is expressed; where the mucous membrane is not protected by the stratum corneum, a large number of leukocytes are noted, which, obviously, is also a manifestation of the protective function of the mucous membrane.
The mitotic activity of the oral mucosa is higher than the mitotic activity of the skin epidermis, and mitoses are expressed in those areas of the mucous membrane where it does not keratinize. This dependence is also determined in pathology. Therefore, the degree of mitotic activity of the epithelium is one of the indicators of the severity of protective processes in the mucous membrane.
Operations for cleft palate
Histochemical research methods have established that the epithelium of the oral cavity is capable of accumulating large amounts of glycogen. Most glycogen is contained in the epithelium of the mucous membrane of the cheeks, soft palate, and floor of the mouth, which is observed already during fetal development. In the epithelium of the hard palate and gums, glycogen is normally either absent or present in the form of traces. Consequently, glycogen accumulates in those areas of the oral mucosa where the epithelium does not undergo keratinization; this dependence persists in pathology. For example, with gingivitis and periodontal disease, keratinization processes weaken and, in parallel, an increase in glycogen content is observed. This suggests that in the keratinizing epithelium, glycogen is a source of epergia or plastic material for the synthesis of keratin.
Nucleic acids play an important role in the life of the epithelium, the largest amount of which is contained in the cells of the epithelial growth zone, which indicates the intensity of metabolism in these cells.
The epithelium is connected to its own layer of the mucous membrane through a basement membrane consisting of a dense network of argyrophilic fibers closely associated with the processes of the cytoplasm of the cells of the basal layer of the epithelium. The proper layer of the mucous membrane is the basis to which the epithelium adjoins. It consists of dense connective tissue and forms numerous projections (papillae) that penetrate the epithelium. The size of the connective tissue papillae varies: they contain vessels that supply the epithelium and nerves. The outgrowths of the epithelium that fill the space between the connective tissue papillae are called epithelial papillae. The latter increase the area of contact between the epithelium and the connective tissue base, which promotes the exchange of substances between them and a tighter connection. The height of the connective tissue protrusions is proportional to the thickness of the epithelium. The highest protrusions are observed in the lips, cheeks, on the back and tip of the tongue. The most dense bundles of collagen fibers are located in the mucous membrane of the gums and hard palate as areas most susceptible to mechanical stress. In a scanning electron microscope, the surface of the cheek epithelium is embossed, penetrated by numerous holes, possibly performing the suction function of the mucous membrane; A clear framework of the vascular network is often visible, and a small number of fibrin strands are constantly detected. The surface of the gum epithelium consists of irregularly shaped cells, penetrated by numerous small pores and holes. The cell boundaries are dense and protrude above the surface of the epithelium.
The proper layer of the mucous membrane passes into the submucosal layer without a sharp boundary. The submucosal layer consists of loose connective tissue; Along with bundles of collagen fibers, there is also adipose tissue. This layer is not present in the mucous membrane of the tongue, gums, or hard palate. The interdental papillae of the gums are formed by loose connective tissue. It contains capillaries and contains many sensitive nerve endings. The own layer of the mucous membrane of the gums and hard palate is immobilely connected to the periosteum of the jaws. Around each tooth there is a periodontal pocket - a slit-like space between the neck of the tooth and the free edge of the gum. The area of the gum that forms the periodontal pocket is covered with multilayered squamous epithelium, which passes to the surface of the tooth neck, forming the so-called epithelial cover; the epithelium here does not keratinize.
Color test for novocaine
If the integrity of the epithelial cover of the periodontal pocket is violated, the periosteal barrier of the tooth is disrupted; In these cases, the periodontal pocket becomes the site where the pathological process begins to develop (gingivitis, periodontal disease).
The mucous membrane of the floor of the mouth, transitional folds, lips and cheeks has a well-developed submucosal layer and is loosely fused to the underlying tissues, which ensures free movement of the tongue, lips, and cheeks.
The mucous membrane of the tongue differs in structure from the areas of the oral cavity described above. On the tongue, the mucous membrane is tightly fused with the intermuscular connective tissue; the submucosal layer is absent. The dorsum of the tongue is covered with unevenly keratinized stratified squamous epithelium; the mucous membrane here is thickened and rough. The lamina propria forms tall projections covered with epithelium. These projections form the papillae of the tongue. The mucous membrane of the lower surface of the tongue is very thin; Loud veins are visible through it; there are no papillae. When the mucous membrane of the floor of the mouth passes to the lower surface of the tongue, a vertical fold is formed - the frenulum of the tongue. In the area where the frenulum is attached to the tongue there is a small elevation on which the ducts of the submandibular and sublingual salivary glands open. On the sides of the frenulum and in front of the excretory ducts there is a fringed stripe. On the back of the tongue there are 4 types of papillae: filiform, mushroom-shaped, grooved, leaf-shaped.
The filiform papillae are the most numerous and have the appearance of cone-shaped elevations. They fit tightly together, and therefore the surface of the tongue has a velvety appearance. Filiform papillae play the role of organs of touch and perform a mechanical function. The epithelium covering the filiform papillae becomes keratinized. Desquamation of the surface layer of the epithelium of the filiform papillae is an expression of the physiological process of regeneration. When the function of the digestive organs is impaired, in general inflammatory, especially infectious, diseases, the rejection of the surface layer of the epithelium of the filiform papillae slows down, the tongue becomes “coated.” There are fewer fungiform papillae than filiform papillae. They are covered with non-keratinizing epithelium. Their greatest number is located in the area of the tip of the tongue. These are the organs of taste. The circumvallate papillae are also organs of taste, numbering 8-15, they are located on the border between the root and body of the tongue, close to each other in the form of the Roman numeral five. They do not protrude above the surface of the mucous membrane. The ridge of mucous membrane surrounding each papilla is separated from it by a deep groove into which small mucous protein glands (Ebner's glands) open.
The epithelium of the papilla contains a taste bud containing a large amount of acetylcholinesterase and acid phosphatase, which indicates their importance in the conduction of taste stimulation. Leaf-shaped papillae in the form of 3-8 parallel folds 2-5 mm long are located at the base of the lateral surface of the tongue. The epithelium of the papillae also contains taste buds. In the area of the root of the tongue behind the blind foramen is the lingual tonsil, which, together with the palatine and pharyngeal tonsils, forms the lymphoid pharyngeal ring. In the area of the tip of the tongue there are mixed mucous glands, which open through several excretory ducts on the lower surface of the tongue.
In all areas of the mucous membrane where there is a submucosal layer, there are small salivary glands in the form of a cluster of glandular cells. The largest number of minor salivary glands are located in the submucosal layer of the lips and soft palate. They are represented by parenchyma, consisting of lobules separated by connective tissue and excretory ducts. The gland ducts have an uneven width. The shape and size of the terminal sections of the excretory ducts are different, and occasionally their retention is observed with the formation of cystic cavities. Our studies revealed the role of these glands in the development of chronically recurrent aphthous stomatitis (glandular form).
Anesthesia of superficial tissues
The so-called Serra glands, found in. mucous membrane, have nothing in common in structure and function with the minor salivary glands. According to N.M. Chuprynina, V.V. Roginsky, V.V. Panikarovsky and S.B. Ilyin, they represent accumulations of epithelial cells. These formations usually resolve after the baby is born, but can also be found in adults. It has been suggested that they play a role in the eruption of baby teeth (they mark the path of the erupting tooth). Serre's glands are dense, slow-moving round formations of a grayish-pearlescent color and have a shiny surface. Their size varies from 1 to 5 mm in diameter, their number is 3-10. They are usually located in the area of unerupted molars and anterior teeth. From a morphological point of view, they are a tumor-like formation in the form of a cyst, the cavity of which is lined with stratified squamous epithelium and contains dystrophically altered cells of the spinous layer of the epithelium, keratotic cells and detrital masses.
In the upper part of the own layer of the mucous membrane in the area of closure of the molars, around the openings of the excretory ducts of the parotid salivary glands, in the retromolar areas and in the red border of the lips, heterotopic sebaceous glands (the so-called Fordyce granules) are sometimes observed. Fordyce granules belong to the nevi of the sebaceous glands and are round, yellowish elements. Individual lobules of sebaceous glands can be located singly or accumulate in areas of epithelial proliferation. Heterotopic sebaceous glands can be involved in pathological processes occurring in the oral mucosa or be the initial zone of damage.
Vascularization of the organs of the oral cavity occurs through the external carotid artery and its branch, the internal maxillary artery, from which in turn arises a number of branches that supply the jaws, teeth and mucous membrane. On the lower jaw, the inferior alveolar artery (a. alveolaris inferior) forms the rami perforantes periodontales et gingivales (feeding the periodontium and gums). The artery of the buccal muscle (a. buccinatoria) nourishes the muscles, the mucous membrane of the vestibule of the oral cavity and the gums of the upper jaw. The gums in the area of the upper molars are nourished by a. alveolaris posterior superior. From a. infraorbitalis feeds the gum areas in the area of premolars and front teeth. The branches of the descending palatine artery (a. palatina descendens) nourish the mucous membrane of the palate. The veins accompanying the arteries flow into the internal jugular vein (v. jugularis interna). The pathways of lymph outflow are similar to those from the teeth to the regional lymph nodes (g. Submentalis and g. submaxillaris).
The soft tissues of the oral cavity, including the mucous membrane, are innervated in the same way as the jaws and teeth, by the second and third branches of the trigeminal nerve - n. maxillaris and n. mandibularis. Branches extend from them, forming dental plexuses (plexus dentalis superior et inferior), giving branches to the dental pulp, periodontium and gum. N. extend from the main palatine node. nasopalatinus, pp. palatini, innervating the mucous membrane of the palate. P. buccinatorius takes part in the innervation of the mucous membrane of the cheek and gums; the mucous membrane of the floor of the mouth and two-thirds of the tongue is innervated by the lingual nerve (rami isthmi faucium, rami linguales). The glossopharyngeus nerve (n. glossopharyngeus), together with the lingual branch of the vagus nerve, innervates the mucous membrane of the root of the tongue.
The cellular elements of the connective tissue of the oral mucosa play an important role in protective immunological processes. They are less differentiated compared to skin connective tissue cells. The bulk of cellular forms are fibroblasts and histiocytes (sedentary macrophages); characterized by the presence of a large number of plasma cells and mast cells. All of them are scattered between collagen fibers, most of them in the circumference of blood vessels.
Fibroblasts are the main cellular form of connective tissue. Their activity is associated with the biosynthesis of collagen fibers and metabolism. Histiocytes are important in the development of immunity and phagocytosis processes. During inflammatory processes, histiocytes turn into macrophages, absorbing bacteria, necrotic tissue, etc. After the end of inflammation, they again turn into resting cellular forms. In specific forms of inflammation, macrophages form cells characteristic of this form of inflammation.
Plasma cells are normally found in the mucous membrane of the oral cavity and the entire gastrointestinal tract, the mucous membrane of the nasal cavity and the respiratory tract. Their presence appears to be an immunological response to the influence of bacterial antigens that normally inhabit these organs. Plasma cells are found in the adventitia of large vessels, in the stroma of the salivary glands, etc. Mature plasma cells contain large amounts of RNA. They carry out protective immunological processes of the mucous membrane - these are the so-called immunocompetent cells.
Mast cells - functional cells of connective tissue - are characterized by the presence of granules in the protoplasm; They are localized along the blood vessels (in their adventitia), nerves, and excretory ducts of the glands. In loose connective tissue they can be located in groups away from the vessels. In the oral mucosa, there are more mast cells in the area of the lips and cheeks, and fewer in the area of the tongue, hard palate, and gums, i.e., there are fewer of them where the epithelium keratinizes. Mast cells are carriers of biologically active substances that are released during degranulation and are triggers for inflammation. When mast cells degranulate during allergic reactions, histamine and heparin are released, causing anaphylactic reactions.
Research by Zh.K. Lopunova made it possible to establish that in humans, mast cells localized in the area of the mucous membrane of the lips, cheeks, and soft palate differ from mast cells localized in the area of the hard palate and gums according to the results of histochemical reactions. In mast cells of the gums and hard palate, heparin sulfo groups were found in the absence of a protein component in the cytoplasm. In mast cells of the soft palate, lips, cheeks and tongue, a complex composition of the carbohydrate component in the presence of protein was revealed. Apparently, the detected different typtorial properties of mast cells localized in different parts of the oral mucosa are due to protein and carbohydrate components. When pathological processes occur in the oral mucosa, segmented leukocytes and lymphocytes appear in it. Histiocytes can transform into epithelioid cells, which in turn can form giant cells. Epithelioid cells are detected in specific diseases of the oral mucosa, candidiasis. When infiltrates appear that accompany pathological processes, its cellular composition has important diagnostic significance.
Pathological processes
Various pathological processes can occur on the mucous membrane, all of them are divided into the following types:
- inflammatory;
- tumor.
Inflammation is the body's response to an external stimulus. It can be acute or chronic. Based on morphological characteristics, three forms can be distinguished:
- alternative;
- exudative;
- productive.
Defects may occur in the oral cavity, depending on influencing factors:
- Superficial . In the form of erosions, when only the upper cover of the epithelium is damaged and the basal layer is not affected. In such cases, complete restoration of the surface after treatment is possible.
- Deep . In the form of ulcers, they affect the epithelial and connective tissues of the oral cavity. After treatment, the healing process occurs, but scars remain.
Any pathological processes affect the condition of the oral surface. Changes occur here that mainly affect the processes of keratinization of the epithelium.
Main pathologies:
- Acanthosis is characterized by an increase in the thickness of the epithelial layer as a result of the proliferation of basal cells and elongation of the interpapillary processes. As a result, nodules may form. The cause of this phenomenon is diseases such as lichen, leukoplakia, lupus, cheilitis, etc.
- Parakeratosis is a phenomenon manifested in incomplete keratinization of cells on the surface with preservation of elongated nuclei. The adhesive substance disappears from the cells and as a result, the resulting scales peel off. The cause may be diseases such as vitamin deficiency, leukoplakia, lichen, various forms of cheilitis, etc.
- Dyskeratosis is a manifestation of abnormal keratinization, in which pathology of keratinization is observed in individual cells. These cells become larger, rounded and have brightly colored nuclei. Further, they take the form of homogeneous acidophilic formations with small granular nuclei and are located in the stratum corneum. Such manifestations are characteristic of Bowen's disease and squamous cell carcinoma.
- Hyperkeratosis is a severe increase in the thickness of the epithelial layer.
This occurs due to the fact that keratin is formed in excess or exfoliation occurs with a delay. The main reason for this phenomenon is increased keratin synthesis due to increased cell activity. Hyperkeratosis can occur due to the following diseases - leukoplakia, lichen, lupus or cheilitis. Papillomatosis disease - Papillomatosis occurs due to the fact that the papillary projections grow and grow into the epithelium. Basically, this phenomenon occurs due to chronic injury to the palate by the prosthesis.
- Vacuolar dystrophy is an internal swelling of epithelial cells with the formation of collapsing cells called vacuoles. The vacuole can occupy the entire space of the cell. The main causes of this pathological process are herpes and lupus.
- Spongiosis is a pathology when fluid accumulates between the cells of the styloid layer. At the beginning of the process, the expansion of the tubules between the cells occurs, which is filled with plasma, and then, with an increase in the amount of plasma, the bonds are broken and a cavity is formed. A blister or bubble appears. This pathology occurs due to herpes, eczema, stomatitis, etc.
- Ballooning dystrophy occurs as a result of disruption of cellular connections in the styloid layer. The reason for this is an increase in the thickness of the epithelium and the appearance of giant cells or their accumulation. In this case, the cell does not divide and floats in the plasma. This pathology manifests itself in herpes, erythema, lichen, etc.
The oral surface requires careful hygiene and periodic examinations for characteristic formations. Any changes in the mouth are a manifestation of one or another disease.
Pathologies in the mouth can be the causes of the following diseases:
- dental;
- venereal;
- skin diseases;
- disturbance in metabolic processes of substances;
- diseases of internal organs;
- diseases of the circulatory system, etc.
Symptoms of dry mouth during menopause
The condition of dry mouth can be identified by the presence of the following symptoms:
- Intense thirst;
- Dryness in the mouth, as well as a sticky feeling;
- The appearance of small cracks on the lip border and in the corners of the lips;
- Feeling of dryness in the throat and nose;
- The tongue becomes stiff, red and itchy;
- Problems with swallowing appear, it becomes difficult to talk;
- The activity of taste buds decreases;
- Hoarseness occurs;
- There may be pain in the throat;
- Bad breath.
A rare autoimmune disease called Sjogren's syndrome has similar symptoms. With it, multiple lesions of all mucous membranes in the body are observed - with severe xerosis syndrome. This pathology mainly develops in women who have entered the postmenopausal period. Its manifestations are a feeling of dryness in the throat and mouth, the appearance of wounds in the corners of the mouth, and a burning sensation in the eyeballs.
[5]