Differential tooth movement
Along the sagittal using extraction
Gaps
There are two reasons for tooth extraction, detailed in Chapter 7:
1) to provide space for straightening crowded incisors without their protrusion;
2) for camouflage of a moderate class II or class III jaw relationship if correction through growth modification is not possible.
The more extraction space required for straightening, the less
space remains for differentiated movement during camouflage, and vice versa.
Rice. 17-11. A unilateral Class II anomaly in an adolescent girl was corrected by unilateral extraction of the upper second molar and unilateral extraoral traction. AD - before treatment. Note the midline shift to the right and the mild skeletal component of the abnormality. E and F - unilateral cervical extraoral traction (for practical reasons, unilateral extraoral traction should be cervical). Notice that on one side (where more tooth movement is needed) the outer arc of the facebow is longer than on the other.
An important part of treatment planning is deciding whether to remove specific teeth and how to close the extraction gaps (by incisor retraction, medial movement of the posterior teeth, or some combination). Orthodontic mechanics depends on this.
Class Il camouflage due to removal of upper first premolars. Like extraction of maxillary second molars, extraction of maxillary first premolars is a deceptively attractive solution to class II problems and should only be undertaken when specifically indicated (see Chapter 8). With this approach, the goal of orthodontic treatment is to maintain the existing Class II molar relationship while closing the space at the site of the extracted first premolar by retracting the protruding incisors (see Figure 17-12). Strengthening the support on the upper jaw is required, but here the use of class II elastic bands is contraindicated. The possibility remains of acting on the first molars through extraoral traction, using a stabilizing lingual arch, or retracting the anterior segment of the maxillary arch through extraoral force acting directly on these teeth.
Rice. 17-11 (continued). G and H - in the process of treatment. I—K—after treatment. Note the midline correction along with the molar relationship correction. L - post-treatment orthopantomogram demonstrates the eruption of the upper third molar in place of the removed second molar. Cephalometric changes were minimal.
Extraoral traction, when used continuously over a long period of time, provides excellent support for the posterior support. The more time a day a patient wears a facebow, the less need for stabilization with lingual blowing.
It seems obvious that a palatal button lingual arch would be more effective than a straight transpalatal lingual arch, but this is not always the case for molar stabilization. The effect of the lingual arch is primarily to prevent mesial-lingual rotation of the molars around their palatal root, and then to prevent their mesial inclination. For preventing rotation, the straight transpalatal archwire (see Fig. 16-35), however, is as effective as a palatal button archwire, and in most patients the stability obtained with a palatal button is not worth the irritation it causes to the palatal mucosa. Note that this is true when using a lingual arch to stabilize molars, but is not true when using it to stabilize premolars, as in the case of second molar extraction described above. With medial traction, the inclination of the molars is greater than their rotation and the presence of a palatal button is necessary for stabilization.
Rice. 17-12. Treatment by extraction of maxillary first premolars to camouflage class II malocclusion. A - profile before treatment. BD —
oral cavity before treatment. E - profile after treatment. FH - oral cavity after treatment. I - cephalometric comparison. In this patient, the retraction of the upper incisors was achieved with good control of the abutment, the esthetic changes were quite acceptable, and the jaw function was normal.
In addition to arch stabilization with a facial or lingual arch, all of the strategies described in Chapter 10 that are used to reduce stress on the abutment (elimination of friction, retraction of canines away from the incisors, etc.) are compatible with the extraction of maxillary first premolars and can be used.
Rice. 17-13. Retraction of the upper canines using a facebow with a J-hook. A - The facebow is attached to the edgewise archwire medial to the bracket on the canine and pushes the canine distally. The force on each side should be about 200 g. B - distal movement of both canines. Please note that at this stage the reaction on one side is greater than on the other, which is not uncommon when the facebow is applied directly to the dentition. C - head cap with J-hooks for canine retraction. D is an alternative head cap design that provides more direct distal force.
Retraction of protruding upper anterior teeth using extraoral traction (see Fig. 17-13) completely eliminates the load on the posterior teeth and from this point of view is extremely attractive7. This technique has two main disadvantages:
1) the system of forces applied to the front teeth is far from ideal. When extraoral traction is applied directly to the anterior segment, it is very difficult to prevent excessive forces from being applied, although the force periodically decreases to zero when the facebow is removed;
2) significant friction is observed not only in places where the teeth slide along the arch, but also inside the facebow mechanism itself.
This makes it more difficult to control the amount of force, and more friction
on one side than the other can lead to an asymmetrical response. In fact, it is not uncommon to see space closing faster on one side than on the other.
Patient cooperation is also important. Only if the facebow is worn almost constantly can effective dental movement be achieved, and although this can be achieved, it is not recommended to rely on this in all cases. Patients must be carefully selected for this method.
In the late 1980s, some dentists stated that removal of upper first premolars resulted in subsequent temporomandibular joint dysfunction. This statement has not been supported by facts and has been refuted by recent research findings8,9. However, it is important to perform extraction of first premolars to camouflage a Class II malocclusion only when indicated.
Removal of upper and lower premolars. Correction of the relationship of the lateral segments according to class II by removing all four first premolars provides that the lower lateral teeth will be moved anteriorly by almost the entire amount of the extraction space. At the same time, the upper jaw will undergo retraction of the protruding anterior teeth without moving the posterior teeth forward. This, in turn, involves (although does not absolutely require) the use of Class I elastic cords to assist in closing the extraction gaps.
Rice. 17-14. The second stage of treatment according to the Begg method, in which inter-arch elastics are used simultaneously with class II elastic cords to close the space and correct the molar ratio. This pattern of elastic forces persists until the extraction gaps close. The effect is to provide anterior movement of the lower posterior teeth by retracting the upper anterior teeth.
The Begg technique is a classic illustration of the use of Class II elastic modules to provide differential movement of the arch segments during molar ratio correction. In the Begg method, light interarch elastics are added at the beginning of the second stage of treatment to assist in space closure while maintaining Class II elastics (see Figures 17-14). A supporting bend is installed on the upper arch in such a way that the upper front teeth are partially deflected back under the influence of the system of forces of the arch itself (see Fig. 16-36).
Rice. 17-15. Scheme of force distribution at the second stage of treatment according to the Begg method, when basic wire arches with supporting bends are combined with elastic interarch modules and class II rods. Support bends provide corpus anterior movement of the molars, as well as lingual inclination of the incisors, which do not receive moments of force. These bends also exert pressure on the incisors and molars, which is counterbalanced by the opposing action of Class II elastics on the upper arch but accentuated by elastics from the lower arch.
On the lower arch, the reference bend is used to control the degree of mesial inclination of the molars. Class II elastic cords enhance and accentuate differentiated dental movements along the arch (Fig. 17-15). Friction as the wires slide along the molar tubes during space closure is minimized by allowing a fairly free passage of the 16 mil base wire in the 25 mil round tube. It is essential to ensure that only light forces are used so that the optimum level of force is provided where bending is required and that the forces for trunk movement are kept below those required.
A similar system of forces can certainly be created using edgewise techniques. The round archwire in edgewise brackets provides incisor inclination in the same manner as the Begg appliance, but the mesial-distal width of the canine brackets tends to maintain the vertical position of the canines, thereby increasing the load on the posterior abutment. Therefore, when closing extraction spaces on both arches using the Begg method, but using the edgewise technique, it is recommended to strengthen the supporting part of the upper arch with a facebow and slightly stiffer Class II elastic cords are required.
Using the edgewise technique, it is also possible to structure the abutment so that space closure by retraction of the upper anterior teeth and anterior displacement of the lower lateral segments occurs without the use of class II elastics. The best control is achieved through a segmental technique using closure loops on each arch that are bent specifically to close that space (see the “Closing Extraction Spaces” section of this chapter).
Rice. 17-16. The cephalometric overlay demonstrates the treatment outcome of the removal of the upper first and lower second premolars. Even with the removal of the second premolar, some retraction of the lower incisors may occur, but most of the space will be closed by mesial movement of the lower molars. This patient's growth was already complete, so there was some downward and posterior rotation of the mandible.
If differential space closure is required without the use of interarch elastics, the more common edgewise approach involves removing the upper first and lower second premolars, thereby altering the abutment strength of the two segments (Figs. 17-16). With this technique, the conventional space-closure technique will move the lower molars forward a greater distance than the upper molars, especially if the posterior maxillary support is reinforced with a stabilizing lingual or facebow. This model for extracting the upper first and lower second premolars greatly simplifies the mechanics of differential space closure using the continuous arch technique.
However, sometimes the mesial displacement of the lower first molars in place of the missing second premolars is quite difficult to achieve. This is especially likely in cases where there is primary edentia of the second premolars and the second primary molar has been removed. This leads to bone resorption, which reduces the size of the alveolar process. In this case, it is recommended to remove the primary molar in parts: first remove only its distal root, leaving the mesial part in the oral cavity (after pulpotomy with calcium hydroxide and temporary filling) until the permanent molar is moved half the required distance, and then remove the second part of the primary molar and complete movement.
©2015-2018 poisk-ru.ru All rights belong to their authors. This site does not claim authorship, but provides free use. Copyright Infringement and Personal Data Violation
The digestive system begins with the oropharyngeal cavity. A tongue is attached to the bottom with its front end, and by throwing it out the frog catches prey. The ducts of the salivary glands open into the oropharyngeal cavity. Their secretion does not contain enzymes and serves to moisten food. Along the edge of the upper jaw there are small conical teeth. The food enters the stomach entirely through the short esophagus, where it is partially digested by gastric juice. Next it enters the small intestine. The bile duct of the liver opens into its initial section, the duodenum, into which the pancreatic duct flows. The small intestine passes into the large intestine, which opens into the cloaca.
Amphibians breathe atmospheric air. The respiratory organs of adult frogs are the lungs and skin. The lungs are paired pulmonary sacs. Their inner surface has a cellular structure, which increases the area of contact with air. The surface of the lungs is densely intertwined with blood vessels. Through the laryngeal-tracheal chamber they connect to the cavity of the oropharynx.
Amphibians do not have a thorax. Ventilation of the lungs is carried out due to the bottom of the oropharynx. When you inhale, the floor of the mouth lowers and the valves of the nostrils open. Air is sucked into the oropharynx. Then the floor of the oropharynx rises, the valves close and air is pushed into the lungs. Exhalation occurs through the mouth when the abdominal muscles contract and the lungs collapse.
Scientific rationale for the modeling sequence of aesthetic restorations
The anatomy of human teeth, their classical features and forms are considered to be well studied for a long time [2, 4]. When using dental materials from previous generations, this knowledge was absolutely satisfactory to dentists. However, the appearance on the market of dental services of ceramics and composites, providing high aesthetic qualities of structures, showed limited information about the fine details of the tooth structure [3, 5]. On the other hand, the insufficiency and lack of demand for medical knowledge in the field of tooth morphology leads to the fact that even classical signs are not always reproduced in the design [7]. The result is more or less pronounced differences in the shape and relief of the restoration from the natural appearance of the tooth.
We studied the aesthetic characteristics of permanent teeth in 350 people using odontoscopy and odontometry.
The need to bite, tear and grind food contributed to the formation of the main groups of teeth: incisors, canines, molars, premolars differ in shape, size, number of roots and are located in the dental arches. The upper arch is usually more rounded, the lower one is slightly compressed in the transverse direction. The anatomical crown, the border of which runs along the neck of the tooth, and the clinical crown, which is located above the gingival edge immediately after the tooth erupts, are identical in height. With age, the anatomical crown shortens as a result of tooth wear. The clinical crown also decreases, but may also lengthen due to gum recession (Fig. 1).
Rice. 1a. Changing the size of the central incisor. Rice. 1b. Changing the size of the central incisor.
Based on general characteristics, teeth were distinguished according to the signs of belonging to the right or left side, which relate to the curvature of the crowns, the ratio of the distal and mesial angles of the crown, and the inclination of the roots.
A sign of crown curvature is a greater convexity of the vestibular part of the crown, located near its mesial edge, and a gentle slope of the distal one. It is more clearly defined when examining the tooth from the occlusal surface and is expressed in 71% of central incisors (Fig. 2).
Rice. 2a. The sign of crown curvature is determined. Rice. 2b. The sign of crown curvature is determined.
In 23% of cases, the convexity is shifted to the distal side, in 6% of teeth the sign of curvature is not detected. The sign of the crown angle characterizes the situation when the mesial angles, composed of the mesial surface and the cutting edge (masticatory surface), are sharper than the distal ones (Fig. 3).
Rice. 3a. There is a pronounced sign of distal deviation of the periodontal dome. Rice. 3b. There is a pronounced sign of distal deviation of the periodontal dome.
This inequality of angles is observed in 85% of central incisors. In molars, the sign of angle is due to more massive mesial cusps. The sign of root inclination means that the root or its apex is curved in the distal direction in relation to the longitudinal axis of the tooth. In the oral cavity, the sign manifests itself as a distal displacement of the apex of the dentogingival dome.
Based on their appearance, teeth were classified into separate geometric shapes (rectangle, triangle, oval), which are characterized by their own characteristics (Fig. 4).
Rice. 4. Basic geometric shapes of permanent teeth.
Rectangular incisors in the absence of abrasion are detected in 55% of cases: the transverse dimensions of the vestibular surface in the gingival, equatorial region and at the cutting edge are close in value, as a result of which the proximal surfaces are almost parallel (Fig. 5).
Rice. 5a. Rectangular cutters. Rice. 5 B. Rectangular cutters.
The angle sign may be weakly expressed. The length of contact with adjacent teeth is significant: in 72% of cases, contact between teeth begins at the apex of the gingival papilla and ends at the cutting edge. With a triangular crown shape, which is characteristic of 39% of intact incisors, the transverse dimensions of the vestibular surface increase from the neck to the cutting edge (Fig. 6).
Rice. 6. Triangular shaped teeth.
The crown angle sign is well expressed in 88% of cases. The length of contact with adjacent teeth is insignificant. The oval shape of the crown occurs in 7% of cases, having similar values of transverse dimensions in the cervical region and near the cutting edge. The largest diameter is at the equator. The lateral surfaces are presented in the form of convex arcs. The corners at the cutting edge are smoothed. Contacts with neighboring teeth are point-like.
The vestibular surfaces of canines, premolars and molars have a more complex geometric shape due to protruding cusps.
According to a survey of young people, in 53% of cases the upper dental arch has an oval shape, in 42% - round, and in these arches there are teeth of any geometric shape: rectangular, triangular, oval. However, the rare rectangular and triangular dental arches (2.6% of cases) are characterized by rectangular and triangular teeth, respectively.
The visual perception of the geometric shape of a tooth can be influenced by the individual characteristics of the dentogingival contour. The dome-shaped gingival margin, characteristic of 56% of incisors, resembles a wedge or triangle in shape and gives the tooth a triangular shape. 39% of incisors have a rounded periodontal edge, 5% of teeth have a flattened, almost straight gingival contour. The shape of the incisal edge also reflects the individual characteristics of the tooth (Fig. 7).
Rice. 7a. The relief of the vestibular surface and scalloped cutting edge are pronounced. Rice. 7b. The relief of the vestibular surface and scalloped cutting edge are pronounced.
Immediately after eruption, the cutting edge is serrated. Then abrasion facets appear. An uneven (convex or concave) surface can be explained by the peculiarity of contact with antagonist teeth.
The relief of the vestibular surface of the tooth is of great aesthetic importance: vertical ridges, bridges, convexities, depressions, and areas. A single ridge is usually characteristic of the middle part of the vestibular surface. If there are two ridges, the most common ones are mesial and distal. The three enamel ridges are usually located mesially, medially and distally (Fig. 8).
Rice. 8a. Vertical ridges on the vestibular surface of the incisors. Rice. 8b. Vertical ridges on the vestibular surface of the incisors. Rice. 8th century Vertical ridges on the vestibular surface of the incisors.
Physiological wear of teeth leads to the formation of a smooth vestibular surface.
Modeling of aesthetic restorations should pursue the goal of reproducing in detail the natural classical, as well as individual characteristics of permanent teeth. However, an analysis of the quality of 145 restorations that were created by reproducing the characteristics of a symmetrical tooth showed differences between the artificial structure and the intact tooth in almost half of the cases [1, 6]. In most cases, this concerns the restoration of rectangular-shaped features where triangular or oval ones are required. In some cases, there is a recreation of oval (rectangular) tooth shapes in a triangular jaw.
The absence of signs of tooth affiliation was found in an average of 30% of restorations. Of these, 77.14% were modeled without taking into account the sign of crown curvature. Many patients had differences in height, width, or asymmetry in the size of individual sections of aesthetic structures (Fig. 9).
Rice. 9a. A veneer differs in size from an intact symmetrical tooth. Rice. 9b. A veneer differs in size from an intact symmetrical tooth. Rice. 9th century A veneer differs in size from an intact symmetrical tooth.
Among the age-related features characterizing the surface relief, there was practically no re-creation of perikymatia on structures in adolescents. The lengthening of the clinical crown of the tooth due to gum recession was not taken into account: the height increased significantly due to the filling material. No gum-mimicking polymers were used.
Individual features of the relief were absent in most restorations (vertical ridges, relief cutting edge).
At the filling stage, insufficient or excessive use of material changed the shape, size, and characteristics of the tooth. Thus, excess filling material on the vestibular surface caused an unnatural convexity of the crown (Fig. 9).
The lack of composite material led to the loss of proper anatomical volume, a decrease in the overall height and proximal slopes, and flattening of the crown. Single structures stood out as a result of asymmetry - differences from a similar tooth on the opposite side. Paired or multiple restorations looked unnatural if a single geometric type of crowns was not maintained, signs of tooth affiliation, and individual characteristics were not observed.
The results of scientific research, including analysis of the aesthetic characteristics of teeth and the quality of existing restorations, made it possible to develop recommendations for step-by-step planning of the sizes and shapes of aesthetic restorations.
The algorithm for planning the size and shape of the structure represents a certain sequence of measuring and describing specific anatomical structures of the tooth (Scheme 1).
Scheme No. 1. Restoration sequence algorithm.
First, it is necessary to conduct a comparative assessment of the size of the clinical and anatomical crown of the tooth. The presence of wear areas in the area of the cutting edge indicates a decrease in the height of the clinical crown. Gingival recession with exposure of the neck and root of the tooth is a sign of an increase in the vertical size of the clinical crown (Fig. 1).
The measurement (odontometry) is made with a micrometer (Fig. 10).
Rice. 10a. Measuring the transverse dimensions of a tooth. Rice. 10b. Measuring the transverse dimensions of a tooth. Rice. 10th century Measuring the transverse dimensions of a tooth.
The height of the clinical crown of the central and lateral incisors is assessed by the distance from the cutting edge to the marginal level of the gums along the vertical midline. Similar dimensions of the canine and premolars are measured along the midline from the apex of the cusp to the marginal level of the gingiva. The height of the molar crown is the distance from the gum level to the top of the most prominent cusp.
The shape of the tooth crown is considered rectangular if the lateral edges of the vestibular surface are parallel, and square if the height and width are equal. Mesiodistal dimensions in the neck of any tooth are measured by the distance between two points of opposite proximal surfaces at the level of the apexes of the interdental papillae. The horizontal parameters of the incisors in the equatorial region are determined at the level of the middle third of the crown height. Similar values of the central and lateral incisors in the area of the cutting edge are assessed by the distance between the protruding points of the mesial and distal edges of the crown. The mesiodistal dimensions of the canines and premolars are measured between the lateral sections of the crown located at the greatest distance. The transverse parameters of molars in the equatorial region are assessed as the distance between the most convex sections of the proximal surfaces.
Visual assessment and measurement results make it possible to describe the geometric shape of the tooth crown based on the relative position of the lateral surfaces.
The shape of the tooth crown is considered rectangular when the lateral edges of the vestibular surface are parallel (square when the height and width are equal). The triangular shape of the tooth is characterized by its maximum horizontal size at the cutting edge. A crown is considered oval in shape when the lateral surfaces have a rounded outline with the largest horizontal dimension in the area of the middle third of the tooth.
Next, the severity of the signs of belonging to the side of the teeth is assessed. The sign of the crown angle is recorded in the case of a predominance of the distal angle of the vestibular surface over the mesial one (Fig. 11).
Rice. 11. No signs of crown angle.
The sign of crown curvature is considered positive if the convexity of the vestibular surface is located closer to the mesial edge. In some cases, there is no sign of crown curvature (Fig. 12).
Rice. 12. Smooth vestibular surface of the central incisors.
A sign of tooth root deviation is noted in the map when there is a distal displacement of the apex of the dentogingival contour. The description of the individual characteristics of the tooth includes the surface topography, the shape of the gingival contour of the tooth, the shape of the cutting edge, and the length of contact with neighboring teeth. The type of relief of the vestibular surface of the incisors is determined by the presence or absence of vertical enamel ridges (Fig. 8).
The shape of the dentogingival contour is assessed by the upper border of the tooth crown, which starts from the top of one interdental papilla, then goes along the edge of the gums and ends at the top of the other interdental papilla (Fig. 13).
Rice. 13. Contours of the gingival dome.
The dentogingival contour can be round, dome-shaped or flat. It is necessary to plan the length of proximal contacts between teeth in such a way that there is enough space for the interdental papilla. The planning stage is completed by choosing the shape of the cutting edge of the teeth (Fig. 14).
Rice. 14. Planning the area of the cutting edge of the central incisors.
The anatomical features of chewing teeth require a careful assessment of the relationship of the cusps on the occlusal surface, and their shape can change significantly due to abrasion. Modeling restorations is a complex and demanding process.
The first stage is the formation of the base of the restoration, which includes the contours of the geometric shape of the dentin and mamelons at the cutting edge, with a clear designation of the lateral and lower boundaries of the dentinal layer (Fig. 15).
Rice. 15. Opaque base of restoration (diagram).
The second stage involves modeling the signs of teeth belonging to the side (signs of curvature, crown angle, deviation of the periodontal dome). The third stage is the reproduction of the individual characteristics of the tooth, including macro- and microrelief, the shape of the cutting edge and the gingival dome. The sequence of restoration of morphological elements corresponds to the sequence of odontoscopic examination and restoration planning. There is a gradual transition from recreating large details (the geometric shape of the vestibular surface) to reproducing medium-sized ones (signs of the angle and curvature of the crown), and then to modeling smaller elements (enamel ridges, teeth in the area of the cutting edge).
Using imaginary lines (two vertical and two horizontal), it is necessary to divide the vestibular surface of the tooth into segments, which will make it possible to more clearly determine the topographic position of a particular morphological element (Fig. 16).
Rice. 16. Conventional division of the vestibular surfaces of teeth into segments.
For example, in the upper tier the dentogingival contour is modeled, as well as a sign of tooth root deviation in the form of a displacement of the top of the gingival dome to the distal side. Predominantly in the middle part of the tooth, a sign of crown curvature is created through the formation of the largest convexity in the mesial region. Individual features of the cutting edge, expressed by varying degrees of transparency and mamelons, are located in the lower tier (Fig. 17).
Rice. 17a. Modeling the basis of the restoration. Rice. 17b. Modeling the incisal edge of the restoration.
Contacts between teeth, proximal slopes, as well as vertical enamel ridges are modeled, respectively, in the mesial and distal parts throughout the middle and lower tier. In the mesial region there may be a median enamel ridge (Fig. 18).
Rice. 18. Modeling of the individual relief of the vestibular surface.
Restoration of large morphological details must be carried out using opaque shades of the composite. The main guideline when working with opaque filling material is the border of the transparent tooth enamel. So, if the enamel evenly covers the entire surface, then for the corresponding layer of filling material it is necessary to leave no more than 0.5 mm of free space around the entire perimeter of the tooth. If the transparent strip is located in the area of the cutting edge, then the opaque is not brought to the lower border by 1.0 mm. In the case where a layer of transparent enamel is observed on the proximal edges, 1.0-1.5 mm should be left for the enamel layer. With severe abrasion, the dentinal layer is formed over the entire height of the tooth crown up to the cutting edge.
During the work, it is necessary to ensure that the thickness of the opaque layers does not exceed the amount of lost dentin. It is important that the opaque layer is not longer or shorter than on a symmetrical tooth and does not interfere with the type of transparency.
In accordance with the algorithm for planning the anatomical shape and relief, developed by the staff of the Department of Therapeutic Dentistry of BelMAPO based on their own odontometric and odontoscopic observations, 166 structures were made.
The results of visual examination of restorations modeled using the technique of preliminary planning of their morphology showed a significant improvement in quality compared to the previous period (see table).
In most cases, the optimal anatomical shape of the teeth was recreated, which corresponded to group affiliation, age and individual characteristics. The frequency of occurrence of signs of angle, crown curvature, and deviation of the gingival dome on restorations has increased almost 10 times. The vertical and horizontal dimensions of the created structures did not differ significantly from intact symmetrical teeth. Thanks to this, a single geometric type was maintained, characteristic of this group of teeth. Age-related features were simulated, including root exposure and age-related abrasion. In the vast majority of young people, enamel ridges and grooves on the vestibular surface were modeled. The alternation of highlights and shadows, due to the presence of macrorelief, emphasized the naturalness of the created restoration (Fig. 19).
Rice. 19a. Planning of aesthetic restorations. Rice. 19b. Modeling of aesthetic restorations.
Thus, the results obtained made it possible to identify errors made in the manufacture of composite restorations regarding sizes, shapes, and surface topography. Inaccuracies were allowed at the planning stage if signs associated with the group affiliation of the tooth, its age or individual characteristics were not recorded.
The lack of a strict sequence of actions, and often the exclusion of the very stage of planning the anatomical shape, caused a significant violation of the aesthetics of restorations. In turn, the use of the proposed algorithm of actions for assessing and reproducing the characteristics of tooth morphology in conjunction with the skills of odontoscopic examination helps to significantly reduce the number of errors and complications during the restoration of the anatomical shape of the restoration.
LITERATURE
- Danilova D.V. // Sat. Proceedings of the 5th Congress of Dentists of the Republic of Belarus. - Brest, 2004. - pp. 138-140.
- Dmitrienko S.V., Ivanov L.P., Krayushkin A.I., Pozharitskaya M.M. Practical guide to dental modeling. - M., 2001. - 239 p.
- Leonova L. E., Zheleznitskikh M. V., Maksimovskaya L. N. // Klin. dentistry. - 2002, No. 1. - P. 8-11.
- Lomiashvili L.M. // Institute of Dentistry. - 2003, No. 2. - P. 6-31.
- Lutskaya I.K. // Modern. dentistry. - 2003, No. 1. - P. 30-37.
- Lutskaya I.K., Danilova D.V. // Sovrem. dentistry. - 2004, No. 1. - P. 22-25.
- Novak I.V., Danilova D.V. // Sat. works of young scientists. - Mn., 2005. - P. 49-51.
What groups are human teeth differentiated into?
The skin plays a significant role in breathing. Through the lungs of different species, from 35 to 75% of oxygen enters and from 35 to 55% of carbon dioxide is removed. 15-55% of oxygen enters through the skin and up to 45-65% of carbon dioxide is removed.
The circulatory system is closed. There are two circles of blood circulation. The heart is three-chambered, consisting of two atria and a ventricle. The arterial cone originates from the ventricle, from which three pairs of vessels sequentially depart: the pulmonary arteries, the aortic arches, and the common carotid arteries.
The right atrium contains venous blood, and the left atrium contains arterial blood. When the atria contract, venous and arterial blood enters the ventricle, where they are partially mixed.
When the ventricle contracts, venous blood is pushed into the conus arteriosus and enters the lungs through the pulmonary arteries. Here gas exchange occurs and arterial blood flows through the pulmonary veins into the left atrium. This is how blood circulation occurs in the small circle. Some of the venous blood is directed to the skin, from where oxygenated blood enters the right atrium.
With further contraction of the ventricle, mixed blood is directed from the conus arteriosus into the aortic arches, and arterial blood into the carotid arteries. Having given oxygen to the internal organs, the blood collects in the right atrium. Thus, when blood moves through the arteries of the systemic circulation, mixed blood flows to the internal organs and arterial blood flows only to the brain.
The excretory organs are a pair of primary kidneys. They are located on the sides of the sacral spinal column in the form of compact bodies. A pair of ureters coming from them opens into the cloaca. Urine, entering the cloaca, flows into the bladder, from where it is periodically released through the cloacal opening to the outside. Some of the dissimilation products are released through the skin.
In connection with the transition to a terrestrial lifestyle, a number of changes occurred in the structure of the nervous system. The size of the forebrain has increased significantly and it is clearly divided into two hemispheres. Clusters of nerve cells appear in the roof of the hemispheres. The midbrain is smaller than that of bony fishes. The cerebellum is small. There are 10 pairs of cranial nerves leaving the brain. The spinal cord has a brachial and lumbar thickening that innervates the limbs. There are 10 pairs of nerves coming from the spinal cord.
The adaptation of amphibian ancestors to life on land influenced the development of sense organs. The eyes are protected from drying out and clogging by moving eyelids and the nictitating membrane. Their cornea is convex, and the lens has the appearance of a biconvex lens. The retina contains rods and cones. Accommodation, as in fish, is achieved by moving the lens relative to the retina.
The organ of hearing becomes more complex. In addition to the inner ear, the middle ear appears. Its cavity is covered from the outside with a thin eardrum. From the inside, it communicates with the oropharynx through the Eustachian tube. Thanks to this, the internal and external pressure on the eardrum is balanced. Vibrations of the eardrum, through the only auditory bone, the stapes, are amplified and transmitted to the oval window of the inner ear.
The olfactory organs play an important role in the life of amphibians and are represented by paired olfactory sacs. They open outward with the nostrils, and into the oropharyngeal cavity with the choanae. The surface of the mucous membrane of the bags is folded, covered with sensitive epithelium and moistened by the secretion of the mucous glands. The olfactory organs function only in the air, because in water the external nostrils are closed.
The organs of touch are numerous sensory receptors scattered in the skin.
Amphibians are dioecious animals. The gonads are paired - ovaries in females and testes in males. The oviducts open into the cloaca, the vas deferens into the ureters. Males also differ from females in external characteristics. Males have vocal sacs - resonators located on the sides of the head. In addition, on the first toe of the front legs there are genital tubercles, which reach noticeable development during the mating season.
Date added: 2015-04-25; ; Copyright infringement?;
Human dental formula
Many people have heard that dentists call teeth by different numbers. Thus, each unit is assigned a specific number, which guarantees maximum accuracy in records of dental conditions or treatment procedures. The count is made starting from the middle of the dentition to the right and left sides. The anterior units - incisors - are No. 1 and 2, 3 - canines, 4-5 - premolars, 6, 7 and 8 - molars, the last of which is the wisdom tooth.
To determine exactly where the tooth is located, the jaw is figuratively divided into segments. The beginning of the numbering is the right side of the upper jaw of the teeth. Units are written as two-digit numbers, where the first determines the serial number, and the other determines the so-called segment. The upper right half of the teeth is designated by numbers 11-18, the left - 21-28, and the lower left segment - 31-38 and 41-48. Regarding primary teeth, the count is made starting from the front units on the left in a clockwise direction. They are assigned the numbers 50, 60, 70 and 80.
READ ALSO: structure of the human upper jaw and functions of its processes
There are several types of numbering that dentists use:
- With the square-numeric Zsigmondy-Palmer method, Arabic numerals are used for radical units, and Roman numerals are used for dairy units. Often used by orthodontists and surgeons.
- Haderup's method is based on the symbols "-" and "+", where the first denotes the lower and the other the opposite arc. Units are written in Arabic numerals, and in the case of dairy units, 0 is added.
- The Viola system uses Arabic numerals 1-8 for units and two-digit numbers for segments. This type is very convenient, which is why it is widely used by dentists around the world.
- The last system is universal. Each group of units is assigned a letter, number and segment number.
Anatomy of the lower jaw
Although the number and names of the teeth in the anterior and lower jaws are the same, they differ in their structure and purpose (we recommend reading: structure and anatomy of the lower jaw). When comparing the upper incisors with the lower lateral incisors, it is worth noting that the lower tooth is smaller in size, and the outer surface has a blunt and sharp edge. In addition, the lower incisors do not have such deep roots and are smaller in size. The shapes of the lower lateral and medial incisor are similar to each other.
The lower canines are identical to their upper tooth counterparts, but differ in their tapered edges. Looking at the molars and premolars of the lower jaw, it is noticeable that the number of tubercles is different and there is one less root.
The characteristic of the first small molar of the lower jaw will be a rounded shape and a flattened flat root. The second one is large in size due to the presence of well-developed tubercles and a horseshoe-shaped fissure.
The lower six, or first molar, consists of two roots and a large number of cusps. The second and third molars are similar to the first.
Upper jaw and its structure
If you compare the lateral upper incisor with the lower one, you will find that the front one is characterized by a flat shape, and the tooth has only one root and a beveled edge. Of all the incisors, the upper medial is the largest. The lateral incisor is externally similar to the central one, but the cutting edge has a convex, streamlined shape. In addition, the lateral (as opposed to the central tooth) incisor is characterized by a smaller size. Teeth belonging to the “canine” group have a single tubercle, and a groove on the inner surface of the unit divides it into two parts.
Premolars, unlike antagonists, are square in shape. Their roots are slightly flattened and a slight bifurcation is noticeable.
The upper teeth include molars - large units, they are assigned the function of chewing food. The first major molar is characterized by a rectangular shape with four cusps. The second molar has a similar structure and functionality, but is slightly smaller. The third is a wisdom tooth; it does not always germinate, which does not threaten any negative consequences.
Evolution of the dentition and oral glands of vertebrates
Fish
The dental system is homodont (teeth are the same). The teeth are conical in shape, facing backwards, serve to hold food, are located along the edge of the skull, and in some cases, on the entire surface of the oral cavity.
There are no salivary glands in the oral cavity, because... They swallow food with water. The tongue is primitive, in the form of a double fold of mucous membrane. The roof of the oral cavity is formed by the base of the skull - the primary hard palate. The mouth opening is surrounded by folds of skin - lips, which are motionless. General oropharyngeal cavity.
The placoid scales of cartilaginous fish are a plate with a spine placed on it.
Which mammals have teeth that are NOT differentiated?
The plate lies in the corium; the apex of the spine protrudes through the epidermis. The entire scale consists of dentin formed by corium cells; the tip of the spine is covered with enamel formed by cells of the basal layer of the epidermis.
Larger and more complex placoid scales are located in the jaws, forming teeth. In essence, the teeth of all vertebrates are modified placoid scales of their ancestors.
Amphibians
The dental system is homodont. The teeth of a number of amphibians are located not only on the alveolar arch; they, like fish, are characterized by polyphyodontism.
Salivary glands appear, the secretion of which does not contain enzymes. The tongue contains muscles that determine its own mobility. The roof of the oral cavity is also the primary hard palate. The lips are motionless. General oropharyngeal cavity.
Reptiles
The dental system of modern reptiles is homodont ; poisonous reptiles have special teeth through which poison flows into the bite wound. The teeth are arranged in one row. Some extinct forms show initial differentiation. All reptiles are characterized by polyphyodontism.
The salivary glands are better developed; among them are the sublingual, dental and labial. The secretion of the glands already contains enzymes.
In venomous snakes, the posterior pair of dental glands are transformed into poisonous ones; the secretion contains toxins (poison).
The tongue is formed from three rudiments: one unpaired and two paired, lying in front of the unpaired one. The paired primordia later grow together. In most reptiles this fusion is incomplete and the tongue is forked.
The rudiments of the secondary hard palate appear in the form of horizontal bone folds of the upper jaw, which reach the middle and divide the oral cavity into the upper section - the respiratory (nasopharyngeal) and the lower - the secondary oral cavity. The lips are motionless.
Mammals
The teeth are heterodont , i.e. differentiated: there are incisors (incisivi), canines (canini), small molars (praemolares) and molars (molares). In pinnipeds and toothed whales, the teeth are not differentiated. The teeth sit in the alveoli; on the alveolar arches of the jaws, the base of the tooth narrows, forming a root.
The incisors and canines are very similar to the conical teeth of their ancestors (reptiles); the molars underwent the greatest evolutionary transformations and first appeared in beast-toothed lizards.
Due to the differentiation of teeth, the duration of functioning increases. In ontogenesis, there are two changes of teeth ( diphyodontism ): incisors, canines and molars have two generations (deciduous and permanent); small radicals - only one.
The total number of teeth varies among different orders: for example, elephants have 6, wolves 42, cats 30, hares 28, most primates and humans have 32.
The salivary glands of mammals are numerous: these are small ones - lingual, buccal, palatal, dental - homologous to the glands of reptiles, and large ones - sublingual, submandibular, parotid. Of these, the first two appeared as a result of differentiation of the sublingual gland of reptiles, and the parotid glands were a new acquisition of mammals. In the oral cavity - in higher mammals, large accumulations of lymphatic tissue - tonsils - appear.
Language, like that of reptiles, develops from three rudiments. The secondary hard palate becomes continuous, the oral cavity is completely separated from the nasal cavity, thereby achieving independence of the functions of the oral cavity and breathing. Posteriorly, the hard palate continues into the soft palate - a double fold of mucous membrane separating the oral cavity of the pharynx. The transverse ridges of the hard palate contribute to the grinding of food. In humans, they gradually disappear after birth.
The lips of marsupials and placentals are fleshy and mobile, which is associated with feeding the young with milk. The lips, cheeks and jaws define a space called the vestibule of the mouth.
Humans have a dental formula of 2123
2123 (half of the upper and lower jaw).
The teeth, compared to other primates, have decreased in size, especially the canines; they do not protrude from the dentition and do not overlap. Diastemas (gaps between teeth) in the upper and lower jaws disappeared, the teeth became in a dense row, the dental arch acquired a rounded (parabolic) shape.
The molars have a four-cusped shape. The last pair of molars, “wisdom teeth,” erupt late—up to 25 years of age. They are clearly vestigial, reduced in size and often poorly differentiated.
During chewing, the lower jaw can perform rotational movements in relation to the upper jaw, due to the non-overlapping of the reduced canines and the complementary cusps of the chewing teeth of both jaws.
Atavistic anomalies of the human oral cavity:
a) a rare anomaly - homodont dental system, all teeth are conical;
b) tricuspid molars;
c) eruption of supernumerary teeth, i.e. in humans it is possible to form more than 32 tooth germs;
d) absence of “wisdom teeth”;
e) a very rare malformation of the tongue - bifurcation of its end, as a result of non-fusion of paired rudiments in embryogenesis;
f) disruption of the fusion (this should occur by the end of the eighth week of embryogenesis) of the horizontal bone folds that form the hard palate, leading to non-fusion of the hard palate and the formation of a defect known as the “cleft palate”;
g) a cleft of the upper lip (“cleft lip”) occurs due to incomplete fusion of the dermal-mesodermal processes that form the upper lip, two of which (lateral) grow from the upper jaw, and one (central) from the frontonasal process.
Mammalian teeth vary in structure and function. The teeth are located in special alveoli (cells), and can be divided into molars, subradicals, canines and incisors according to their structure and type of functions performed. Almost all mammals first grow baby teeth, which have no roots. Then the milk teeth are replaced by permanent teeth that have roots. This process happens once in a lifetime. Teeth are made of durable tissue - osteodentin , covered with enamel .
The feeding pattern of mammals determines the animal’s dental system. Predators have well-developed canines, in the upper jaw there is the last false molar, and in the lower jaw - the first molar, which have a sharp cone shape. Most herbivorous mammals do not have fangs at all. Ruminant mammals do not have incisors on the upper jaw. Rodents have incisors that do not have roots, so that the incisors, which are ground down on trees and plants, can grow throughout their lives.
Moreover, constant grinding of the incisors on wood or plants contributes to greater sharpening of the teeth.
Biochemical composition
In a child and an adult, each organ of the dentition on the upper and lower jaw consists of calcified tissue, and the main one is dentin, covered with enamel. Each part of the tooth is different in composition; they have a unique functional purpose and biochemical composition. The main components include minerals, inorganic compounds, organic compounds and water.
Wet mass percentage:
- enamel consists of 2.3% water, dentin 13.2%, pulp 30%, cement 36%;
- 1.7% enamel consists of organic compounds, 18.5% dentin, 39% pulp, 21% cement;
- enamel consists of 96% inorganic compounds, dentin 69%, pulp 25%, cement 42%.
The basis of the dry mass is calcium; the tissue also contains magnesium, phosphorus, potassium, sodium and other trace elements. The organic components of the tooth are organic acids, proteins, hormones, lipids, enzymes, vitamins, and nucleic acids.
The main part is soluble and insoluble proteins. Soluble ones perform mainly protective, thermal, transport and other functions. The largest amount of globulin and albumin is concentrated in the pulp, and it also contains glycolytic enzymes and tricarboxylic acids. The main soluble enzymes of the pulp are acid and alkaline phosphatase; they take part in the direct mineral metabolism of organ tissues.
Class Mammals
General characteristics of the class of mammals, characteristics of mammals, features of the class, representativesClass MammalsReply left by Guest
The differentiation of teeth reflects the differentiation of their functions in certain animals. The teeth themselves, which appeared in fish, are also found in reptiles and mammals. They are lost in birds. The question of differentiation of teeth in fish and reptiles (if we do not consider venomous snakes) is debatable. In mammals, we observe different types of teeth. The functions of the teeth are: capturing, holding, tearing and chewing food.
What are differentiated teeth?
According to their structure, they are usually divided into: incisors, canines and molars. In some mammals, the latter are divided into premolars (premolars) and molars proper. Depending on the food specialization of certain families, orders, species and other taxa, certain types of teeth are developed or reduced. In addition, different taxa have different numbers of teeth for certain functions, and the teeth themselves are often very specialized. For example, herbivores often have very developed incisors, for cutting grass or leaves, and molars, for chewing rough food. At the same time, their fangs are very often reduced. In predators, on the contrary, fangs are quite developed, since they allow them to bite through the integument of the victim and hold it. Rodents have developed incisors, especially the upper ones, and in unspecialized, omnivorous animals, which include humans, all of the above types of teeth are present, but without a strongly pronounced specialization, such as in rodents. Thus, we can most clearly observe the differentiation of teeth in various mammalian taxa.
Intussusception of teeth or “Tooth in tooth”
Dental intussusception (dens invaginatus), also known as dens in dente, is a rare anomaly.
This condition means that the outer hard tissues of the tooth have penetrated into the pulp. This article discusses the current treatment protocol for dental intussusception in a 13-year-old girl. As with most cases, early diagnosis and preventive measures help minimize complications associated with dental intussusception. Dental intussusception (dens invaginatus), also known as “tooth in tooth” (dens in dente) is an anomaly of embryological origin. On an x-ray, this anomaly sometimes looks like a tooth within a tooth, which is the reason for its name. Synonyms: invaginated odontome, dilated gestant odontome, dilated composite odontome, dentoid in dente and tooth inclusion.
Radiographic examination demonstrates that enamel and dentin can penetrate deep into the pulp cavity, root, and even the root apex. This malformation was first described by Ploquet in 17943 using the example of a whale tooth.
According to Hovland and Block, the incidence is in the range of 0.04% -10%. Invaginations can occur in any tooth, affecting both the primary and permanent dentition6, but they typically occur in the upper lateral incisors6,7. In some patients, bilateral symmetrical occurrence of intussusceptions has been reported, which suggests that if intussusception is present on one side, it is necessary to examine the opposite side. Intravaginations were rarely found in molars, premolars, and central incisors of the maxilla. Of the total number of detected invaginations, 43% were found in the lateral incisors of the maxilla. The cause of intussusception is unclear; however, some evidence suggests a hereditary component.
This report describes a case of unilateral intussusception in a maxillary lateral incisor.
Description of a clinical case
A 13-year-old girl was referred to the Department of Pediatric and Preventive Dentistry at Rural Dental College and Hospital, Loni, India, with the chief complaint of recent swelling in the right anterior maxilla. The patient described diffuse swelling in the right anterior cheek area, which resulted in elevation of the nasal ala. During an intraoral examination, a depression was found in the lateral incisor of the upper jaw, slight discoloration of the crown was observed, and the tooth responded positively to vertical percussion. The radiograph revealed intussusception of the right maxillary lateral incisor with radiolucency in the apical region (Fig. 1A). A diagnosis of type III (Oehlers) tooth intussusception with dentoalveolar abscess was made.
Intraoral radiographs and CT scans were used for diagnosis. A computed tomography study showed complex tooth anatomy with multiple canals. The distal canal was C-shaped and opened medially. The palatal canal was located distally, and the central canal extended to the depth of the intussusception (Fig. 1B and Fig. 1C).
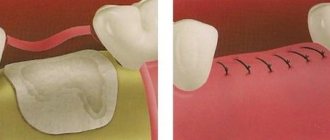
Magnification was used to make channel searching easier. Access to the pulp chamber was gained and an x-ray was taken with a K-flex file No. 10 in the canal. The working length was determined using K-file No. 10 (Figure 1D), mechanical treatment of the canals was carried out with K-file No. 35. Since conservative treatment of the apical region of one of the canals was difficult, we planned apical surgery and retrograde filling with MTA (mineral trioxide aggregate) with obturation with thermoplasticized gutta-percha. The results of regular blood tests were within normal limits. At the subsequent appointment, the tooth was prepared for surgery. During the operation, the mucoperiosteal flap was detached and a hole was made in the projection of the apex (Figure 1E). After complete curettage of the soft tissues and subsequent removal of granulation tissue, correction (grinding) of the hard tissues of the apex was performed. After thorough cleaning, a retrograde MTA filling (ProRoot®, DENTSPLY, www.denstply.com) was performed (Figure 1F), followed by obturation with thermoplasticized gutta-percha ( [email protected] , Cordless Obturation System, DXM, Korea, www.dxm.co .kr) (Figure 2A). The flap is placed in place, the wound is sutured with 5-0 silk thread.
At a follow-up visit one week after surgery, the suture was removed and healing proceeded without complications. 1.5 months after treatment, the patient had no complaints. On the control radiograph, signs of hard tissue regeneration in the periradicular area can be assessed (Fig. 2B). Follow-up radiographic examination performed 6 months later showed complete recovery.
The use of thermoplasticized gutta-percha to fill intussusception facilitates the procedure and provides more effective filling, which is what we did in this study.