Clasps for dentures are part of an artificial structure that ensures its fixation and support. It is a small hook that covers the adjacent tooth.
Manufacturing
Clasps for dentures are made by stamping, casting, and also using forceps and special wire. Plastic clasps are mainly made using the casting method. Stamped varieties are made from metal alloys. Using special wire tongs, bent-cast types are made. Since the hook consists of a process, a shoulder and a body, for this you will need to make 3 bends. To make a shoulder, bend the end of the cast wire, then make a bend and form the body of the clasp.
The support-retaining type of fixator, in addition to the shoulder and body, also consists of an occlusal pad and an anchor part. The lining is located in the intertubercular groove. When the tubercles are very pronounced, it keeps the tooth from moving in the event of an angular force acting on it. An anchor is used to connect the structure to the metal frame.
What does a clasp consist of?
Let's start with retention clasp, as it is simpler. It has 3 parts:
- 1 – shoulder – holds the clasp on the tooth
- 2 - body - connects the shoulder and process
- 3 - process - holds the clasp inside the prosthesis
support-retaining is more complex .
We will analyze it using the example of the classic Acker clasp (1st clasp of the Ney system) in which the following parts are distinguished
- shoulder;
- occlusal pad;
- clasp body;
- clasp extension.
The shoulder is the part of the clasp that holds the clasp on the tooth.
The occlusal pad (foot) is the third short arm of a triangular (oval) clasp. It lies on the occlusal surface of the tooth and is needed to transfer the chewing load to the tooth.
The body of the clasp is the junction of all its elements.
The clasp extension (connecting rod) is the rod with which the clasp is connected to the prosthesis. The length and shape of the process depends on the type of connection between the prosthesis and the clasp.
Classification
Clasps are classified by material. They are:
- plastic;
- metal: chromium-cobalt, gold-platinum and chromium-nickel;
- metal-plastic.
- tape;
- round;
- semicircular.
- dental;
- gingival;
- dentogingival.
- ring-shaped;
- changeover;
- T-shaped;
- one-shoulder;
- double shoulders;
- double;
- multi-link.
- articular and labile;
- springy and semi-labile;
- rigid or stable.
The shapes of clasps are:
According to their performing functions, they are divided into holding and supporting-holding.
According to the place of contact, clasps for dentures are classified into:
Depending on the degree of coverage of teeth, these structures are:
Clasps are classified according to the method of connection to the prosthesis base. They are:
Plate dentures with clasps according to Kemeny
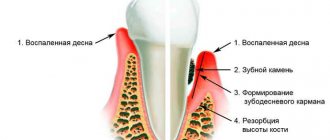
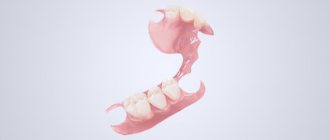
Metal clasps and other types of mechanical fastening of a prosthesis on the jaw have a number of disadvantages (they violate aesthetics, have a harmful effect on the hard tissues of the tooth and periodontium, their use often involves covering the teeth with metal crowns). In this regard, claspless prostheses or various designs of plastic clasps, devoid of the disadvantages inherent in metal ones, have found widespread use. This issue was most fully developed by the Hungarian dentist I. Kemeny, and the plastic clasps he proposed are called retention clasps. The dentoalveolar clasp consists of two parts (alveolar and dental), directly transforming into one another and located according to their names (the alveolar part is vestibular as a continuation of the artificial gum, above the transitional fold; processes extend from it against the outer 2-3 teeth, ending in a T-shaped cleft adjacent to the surfaces of the crowns of the teeth, slightly below the equator). Technique for making a denture with a dentoalveolar clasp. On the working model, the boundaries of the prosthesis base and the location of the alveolar and dental parts of the clasp are drawn with a pencil. After molding the base plastic in the area of the toothless alveolar part (process) and control pressing, the cuvette is opened and additional molding is carried out with white or colorless plastic at the location of the dental part of the clasp. The use of rigid dentoalveolar clasps is possible only with a steep or flat slope of the alveolar part (process) and high clinical crowns of abutment teeth. The disadvantage of this type of clasp is the impossibility of activating it, low strength and insufficient fixation of the prosthesis. The listed disadvantages can be significantly reduced by using elastic plastic, especially with a niche-shaped vestibular surface of the alveolar part (process) and vestibular displacement of the anterior teeth. Pelots are modified alveolar clasps that are connected to the base of the prosthesis using two wires located vestibularly between the necks of the teeth and the transitional fold. Pelot production technique. After modeling the wax base in the area of the toothless alveolar part (process), two parallel and spaced wires 0.6-0.8 mm thick with flattened ends and notches for strengthening in plastic are fixed on the vestibular surface. The wires should be 0.5-0.7 mm from the surface of the alveolar part (process) and their ends should be located on one side in the base of the prosthesis vestibular, on the other - in a plastic sheet measuring 1X0.8 cm (depending on the height of the alveolar part or process). When gypsuming into a ditch, the wires are covered with plaster to fix them on the model and prevent displacement during molding of the plastic.
Retention clasp
Retaining clasps for dentures are a hook that is placed near the neck of the tooth. There are 2 types - alveolar and dentoalveolar.
The classic support-retaining clasp consists of 2 arms. The design also has a process and an occlusal pad. The best representative of this type of clasp is the Ney system. In most cases, the clasp breaks near the base of the prosthesis. The body and upper shoulder part are hard and thick, which is why they began to place it above the center line. As a result, the prosthesis itself does not move sideways, and the installation has become reliable. The thin bottom part also serves as support. This was made possible due to a lower location than the boundary line.
What types of clasps are there?
There are 3 types in total, of which 2 main ones:
- holding;
- support-holding
(3rd type - support clasp, used as an auxiliary clasp together with the support-retaining one)
(The figure shows an example of a support clasp)
Retaining clasps are needed only to hold the denture in the mouth. They are used in plate prostheses.
Support-retaining clasps, unlike support clasps, transfer part of the chewing load to the tooth.
A prosthesis with this type of clasp is called semi-physiological . Such dentures are more comfortable and easier to get used to. (Read more in our article)
Ney's clasp system
This is one of the best artificial structures of its kind. The Ney system clasp has an important advantage - there is no need to use crowns. Therefore, a healthy tooth is not injured during grinding; when chewing food, the load is distributed to the chewing teeth. The denture is fixed with several fasteners, each of which is located in a specific place to hold the product in one position.
The advantages of this product are:
Lock type 3, 4 and 5
Type 3 fasteners combine Acker and Roach fasteners. One shoulder has a T-shape, the second is located next to the chewing area. Clamp 3 is recommended to be used when the dividing line is uneven.
Type 4 latch is called reverse-acting. It is used when small molars and canines are inclined, as well as when there is low support.
Type 5 fasteners are also called single-arm ring fasteners. It is recommended to use it if single teeth are positioned obliquely. The body is supported and completely surrounds the tooth. The main disadvantage is the fragile retention of the prosthesis, therefore discomfort may occur when chewing solid food.
The location of the Acker clasp (Ney-I) depending on the inclination of the tooth crown
This clasp is the most common of all types, because... its design is simple and prevents displacement of the prosthesis in three directions - vertical, sagittal and transversal.
In this case, the onlay is located on the occlusal surface perpendicular to the longitudinal axis of the tooth in both vertical and inclined positions of the molar crown. The body of the clasp is located on the distal occlusal surface of the molar approximately at a right angle to the axis of the occlusal pad. When the tooth is tilted, the area occupied by the clasp body increases, thereby improving the stabilization of the prosthesis. The arms of the clasp start from its body and are directed at an angle of about 45° along the occlusal surface of the tooth until it intersects with the boundary line, after which it continues into the gingival zone.
Acker clasp arm consists of three parts: support, intermediate and retaining.
The supporting part is the most rigid, located in the occlusal zone, covers the tooth, helping to stabilize the prosthesis on the jaw.
The retaining part is elastic, located in the gingival zone and ensures fixation of the prosthesis. The length of the holding part is approximately equal to 1/3-1/2 the length of the arm, i.e. The retention function is performed only by the distal ends of the vestibular and oral shoulders. Between these two parts there is a semi-rigid intermediate part located in the area of the boundary line and crossing it.
The covering (stabilizing) parts of the clasp arms should surround the tooth by more than 180°, and the retention ends should, if possible, reach almost to the adjacent tooth.
The shoulders of the clasps transfer the horizontal component of the chewing load to the supporting teeth.
The Acker clasp is used for defects that are included and in cases where the line of sight divides the vestibular and oral surfaces of the tooth approximately in half. The first type of clasp is not used when the boundary line is located high on the contact surface of the tooth facing the defect. The fixing properties of the shoulder of this type of clasp will be maximum with an undercut depth of 0.5 mm.
Disadvantages of the Acker clasp that limit its use:
• the shoulder covers a significant surface of the tooth, on which food can be retained;
• elastic properties of the retaining end of the arm are limited;
• used only on molars.
The second type is an elastic support-retaining clasp, which has one occlusal pad and two T-shaped split ends of the arms ( Roach clasps ), so it is sometimes called a split clasp.
Roach's Clammer (Ney-II)
In 1930, Roach described 6 types of rod arms of clasps, which formed the basis for the design of one-piece clasp dentures. The most common is the Roach clasp with two rod arms.
The rod arms of clasps can be used on one or both sides of the abutment tooth. The rod arm branches off from the frame below the level of the gingival margin, crosses the area of the clinical neck of the tooth without touching the mucous membrane of the alveolar process, and continues in the vertical direction until it comes into contact with its gingival zone. The beginning of the rod arm and its vertical part must have a relatively large cross-section so as not to break.
Roach clasps must be made of materials that ensure their elasticity and strength. Gold-platinum and cobalt-chromium alloys meet these requirements.
Some authors compare the spring action of Roach clasps with T-shaped arms with pressure distributors and recommend the use of such clasps for defects in the dentition without distal support. The rod arms of Roach clasps, due to their close location to the neck of the tooth, have the property of a latch, i.e. have greater resistance to removal than to insertion of the prosthesis onto its bed.
Unlike the Acker clasp, in which the occlusal pad, body and more than half the length of the arms are located above the boundary line and provide the functions of support and coverage, in the Roach clasp only a small retention part of the core arm is in contact with the gingival zone of the tooth. Therefore, to stabilize the clasp denture on the jaw, the occlusal pads of Roach clasps must be powerful enough. In addition, along with these clasps in the prosthesis, it is advisable to use other, more rigid systems, for example, Akker.
It is recommended to choose this clasp when the boundary line is diagonal and when it is located high (close to the occlusal surface). It is advisable to use the Roach clasp with an undercut depth ranging from 0.5 to 0.75 mm. For large undercut depths, it is also necessary to use a clasp with good springing properties.
The use of Roach clasps alone in the design of a clasp prosthesis, due to the spring action of the rod shoulders, relieves the load on the supporting teeth, but, on the other hand, increases the load on the alveolar process. Therefore, when the alveolar process is not expressed, the use of Roach clasps alone is inappropriate.
Roach clasps have the following advantages:
• provide good retention in various areas of the supporting teeth;
• more effective than Acker clasps in aesthetic terms, because located on the gum side and most of their length is not noticeable;
• the likelihood of caries is reduced, because food remains are retained under long arms that do not contact the tooth surface;
• precise adjustment of the retention end of the rod arm in contact with the tooth is relatively simple;
• effective for teeth with a slight equator and inclined teeth, as well as for short teeth with limited retention capacity;
• as a result of tooth abrasion, the boundary line may be located so close to the occlusal surface that there is no room left to place the shoulders of the Acker clasp; This problem is solved by using clasps with elongated arms.
Disadvantages of Roach clasps:
• cannot be used for pronounced bony protrusions and ridges of the mucous membrane that interfere with the position of the shoulders;
• the rod arm of the clasp does not have a rigid part in contact with the tooth. Therefore, it is less effective than the Acker clasp;
• cannot be used when the gums are exposed when smiling;
• may be accidentally bent by the patient.
The third type is a combined clasp, consisting of a rigid arm with an occlusal pad (like the Acker clasp) and an elastic arm of the Roach clasp. The clasp is used on premolars, molars and canines at different levels of the boundary line on the tooth surfaces. In this design, the holding arm is the rod arm of the Roach clasp, which can be located on the vestibular or oral sides, depending on the inclination of the tooth. When the abutment tooth converges (on the lower jaw), Roach's shoulder is located on the lingual side, and Acker's shoulder is located on the vestibular side. When the abutment tooth diverges (on the upper jaw), on the contrary, an Acker shoulder is made on the palatal side, and a Roach shoulder is made on the buccal side. Consequently, the rigid shoulder is located on the surface where the line of sight is low (close to the gingival margin), the elastic shoulder is located on the opposite side, where the line of sight is close to the occlusal surface.
Swenson and Jackson design
The clasp used on canines is called the Swenson design. This design creates the correct load on the supporting teeth. This is very important during their mobility. The disadvantage of the design is that there must be a gap between the molar and premolar to secure the anterior shoulder.
A reversible clasp is a type of Jackson support-retaining device. The product has 2 branches and bodies. The structure is made by cast and bent method in the shape of a loop.
Classification: types and features of clasps
Fixators are different depending on the prosthesis, material, and functions performed. The most popular clamps include:
- Bonneville. It consists of two onlays that are fixed in the fissures of molars and premolars. They are used for unilateral missing teeth.
- Jackson. Reversible design, which is a loop. Can be cast or wire.
- Dentoalveolar. Made of plastic, reinforcement possible. It is used when it is necessary to achieve an aesthetic effect.
- Round one-shoulder. They are usually folded onto the molars.
- Schwartz. It bends out of the orthodontic wire and occupies the interdental space. It can be single-link or multi-link.
- Adams. A button lock, consisting of two fixing protrusions, curved towards each other, and two bodies, on the inside turning into processes.
- Duisings. It is bent like a Jackson clasp, but has two semicircular bends at the shoulder, two bodies and two appendages.
- Reichelman. It differs from others in the shape of the lining, which looks like a transverse bar, which goes through the chewing surface into the inside of the oral cavity.
There is a classification according to Ney's system:
- Akers. This is a double-arm clamp with an onlay used when the center line is positioned in the middle of the coronal portion.
- Roach. It has a T-shaped shoulder connected by an arc to the body. Used for abnormal deviations of the dental equator.
- Akkera. A combination of the two previous types.
- One-shouldered. It is used on both sides of the jaw, since the fixation is one-sided, and is located in the mesiolingual part of the prosthesis.
- Circular. Located on single molars, covering the entire circumference. Provides unidirectional shifting, therefore it is used on both sides.
Clasp dentures
A clasp denture with clasps is a product with a metal frame. An acrylic or nylon base and artificial teeth are fixed to it. This type of prosthetics in the absence of several teeth is considered one of the most popular.
The advantages of a clasp denture with clasps include:
The clasp denture on the lower jaw does not fall out when talking or chewing food. This became possible thanks to the presence of a splinting structure with hooks, which further strengthen the teeth with increased mobility.
One of the disadvantages is the low aesthetics, because the hooks are visible, especially if they are on the front teeth. Under their influence, supporting teeth may begin to collapse. Since the hooks rub the mucous membrane, it takes a long time to get used to the clasp denture on the lower jaw.
Multi-link clasp
Multi-link clasp The design of a clasp prosthesis sometimes includes a multi-link (orally located) clasp. Most often, such a clasp is used for defects in the dentition in the absence of distal supports. The effect of a multi-link clasp is manifested in the fact that it somewhat absorbs the vertical load falling on the prosthesis—it prevents the prosthesis from settling if the clasp links are located above the dental tubercles of the front teeth. An oral clasp strengthens the prosthesis, so when using it, the clasp can be made thinner and narrower. A multi-link clasp provides some horizontal relief of the supporting teeth; this quality deserves special analysis. The diagram shows the action of a continuous clasp during loading. The position of the horizontal displacement of the clasp prosthesis to the left is conventionally taken. In this case, the load falling on the supporting teeth is transmitted by the vestibular arm of the clasp placed on 4| and the oral arm of the clasp placed on |4. A continuous clasp acts differently in different areas. The group of frontal teeth on the side where the prosthesis moves (the degree of movement depends on the severity of the toothless part of the alveolar process and the compliance of soft tissues), in our example 3 2 1 |, take on part of the load, at the same time |l 2 3 any the load is not perceived. A continuous clasp will have the opposite effect if the clasp denture moves to the right. Taking into account the above, it should be assumed that if the supports that perceive the horizontal load through a continuous clasp are not sufficiently resistant to the load, then these supports will also become loose. Reducing the load is possible by blocking all remaining teeth 4321 | 1234.
The foregoing gives reason to believe: 1) crushers of chewing loads are applicable only in cases of damage to the dentition, characterized by the absence of both distal supports; 2) in the absence of both distal supports, instead of load crushers, it is permissible to block a group of teeth - the block must have endurance equal to the possible load from four antagonist teeth; 3) in cases where one of the distal supports is preserved, the effect of the load-bearing force is counteracted by the placement of an additional clasp on the distal support. If there is a distal support, the outer teeth adjacent to the defect on the side where there is no distal support should be blocked with crowns or clasps. The teeth included in the block, subsequently united by a clasp, must be able to withstand a chewing load equal to the force of four antagonist teeth. If one of the distal supports is retained, the use of load crushers is not justified; 4) some horizontal unloading of the supporting teeth is possible using a continuous clasp. Stabilizers. When there are no distal supports, especially in the upper jaw, sagging of the clasp denture in the posterior region is observed. This is especially pronounced with significant atrophy of the alveolar processes. In such cases, so-called stabilizers can provide some stabilization of the clasp denture on the jaw. Stabilizers, while having a positive value, nevertheless complicate the design of the prosthesis, making the prosthesis more bulky and less comfortable for the patient. In addition, stabilizers can displace the labial teeth on which they rest. This occurs under the influence of constant shocks to all supporting teeth, which are formed during the processing of food in the mouth. These shocks move the teeth on which the stabilizers are located: they act like an orthodontic apparatus.
Dentoalveolar clasp
Plastic is used to make a dentoalveolar clasp. This type of fastener is indicated for anterior teeth. To make it more reliable, the plastic is reinforced with wire. Although this makes the structure stronger, the quality of the material deteriorates. How much dentures cost is directly influenced by the type of design and material of manufacture.
The disadvantages of a dentoalveolar clasp include the fact that it causes the lip to protrude forward. It must not be used for supports with a low crown and alveolar process. Reuse of records is not permitted.
Technique for bending a double-armed wire clasp.
⇐ PreviousPage 7 of 13Next ⇒This clasp has two arms. The first is located on the vestibular surface, the second on the lingual or palatal surface, counteracting the first.
The double-arm clasp is used in two common forms. In the first form, both arms of the clasp have a common body and process; in the second form, the arms of the clasp and the body are isolated from each other and only their processes are united by a common loop. Such a clasp could be called split.
If the arm of the clasp is extended through the interdental space, placing it on the buccal surface of the adjacent tooth, you will get a so-called extended clasp. It is a mistake to think that lengthening the clasp improves its fixing properties. Only one extreme shoulder remains elastic in these clasps. The other links are essentially the body of the clasp. An elongated, or two-link, clasp is indicated for low stability of the outermost abutment tooth.
A double-arm bent wire clasp can be made in two ways.
The shoulder is bent onto the vestibular surface of the tooth and the body of the clasp on its lateral surface, just like a single-arm clasp. Then, grasping the body of the clasp with crampon pliers, bend the second arm, covering the oral surface of the tooth crown, with round-nose pliers or shaped pliers.
An extension is soldered to the double-arm clasp, the end of which is previously flattened and on which notches are applied for fixation in the plastic base.
However, when soldering, the wire loses its springing properties, which is a negative point. Therefore, the process, together with the occlusal pad, can be modeled with wax, cast and soldered to the clasp, which will transform it from a double-arm bent into a double-arm support-retaining bent-cast clasp.
The second method is that from one piece of wire 5-6 mm long and 0.8 or 1 mm thick, bent in the form of a hairpin, both the vestibular and oral arms of the clasp are bent. The ends are smoothed and polished.
Double wire clasp bending technique.
A double clasp or a clasp with an extended arm covers the vestibular surface of two adjacent teeth that limit the dentition defect, or one artificial tooth and one tooth that limits the dentition defect, which promotes better fixation of the prosthesis and protects the supporting teeth from overload.
The end of a wire with a length of 3-4 mm and a diameter of 0.6 to 1 mm is rounded off with round-nose pliers or shaped pliers, the vestibular shoulder is bent onto the tooth distant from the defect and the second shoulder - onto the tooth bordering the dentition defect, the body is bent on its lateral surface and the process is bent into the thickness of the base under the artificial teeth. Such clasps of three sizes can be made using Oksman and Sharlykov forceps.
⇐ Previous7Next ⇒