Material requirements
Canal filling has several purposes:
- preventing infection from entering;
- elimination of inflammation in tissues;
- preventing the penetration of tissue fluid.
Materials for filling root canals of teeth must meet a number of requirements :
- do not cause irritation or allergic reactions;
- have bactericidal properties;
- maintain shape and volume after hardening;
- stimulate bone tissue restoration;
- have adhesive ability;
- do not change the color of teeth;
- differ in radiopacity;
- do not have carcinogenic or mutagenic properties.
Endodontic treatment involves filling the root canals.
The materials used are divided into several groups:
- According to physical properties: plastic (pastes), hard (pins).
- According to the functions performed: for sealing (sealers), for filling (fillers).
- Depending on the duration of installation - for permanent or temporary filling.
Cements
Dental cements are a filling material consisting of a powder and a liquid.
When mixing the components, a homogeneous, plastic mass is formed, which after curing acquires a very strong structure. For each type, this hardening rate is individual.
Some composite compositions, for example Citrix, begin to harden within two minutes after mixing, and therefore require certain work skills from the dentist.
There are several groups of cements, which differ in their composition and, accordingly, in purpose.
Phosphate cements
Phosphate-based cements have many advantages, such as:
- non-toxic;
- optimal coefficient of thermal expansion;
- high insulating properties.
However, several characteristic disadvantages - solubility, shrinkage, low chemical and mechanical stability - force them to be enriched with additional components of antimicrobial action.
Polymer cements
Polymer cements have optimal properties for dentistry. They contain polyacrylic acid, which provides chemical adhesion (adhesion) of the filling to the tooth tissue.
Their characteristics are similar to zinc phosphate cements, but they are characterized by better biocompatibility and are practically not subject to dissolution. Such cements are indispensable for the restoration of temporary teeth, since they do not require the installation of a spacer.
Glass ionomer filling materials
Glass ionomer cements represent a whole class of filling material, which is gradually replacing zinc-phosphate and zinc-silicate systems.
They have their own classification:
- for permanent filling (aesthetic, heavy-duty);
- for gaskets, sealing (quick-hardening);
- for filling root canals;
- for fixation (used for prosthetics).
This material has excellent biocompatibility and chemical adhesion to tooth tissue. During the hardening process, a fluorine release reaction occurs, which causes tissue mineralization and promotes the formation of an antibacterial environment.
Main representatives:
- Fuji cement line – for permanent, restorative filling;
- Filtek is a light-curing material for aesthetic restoration and restoration of chewing molars;
- Core Max – for restoration of the crown part of the tooth;
- Estelite – radiopaque composite for restoration of anterior and lateral teeth;
- Time Line – used for insulating pads under fillings.
Plastic pastes
Plastic materials can be non-hardening or hardening.
Non-hardening agents
This material for filling root canals has a therapeutic effect. It is assumed that when the desired result is achieved, it will be deleted. The product is injected, closed with a sterile cotton ball and a temporary filling.
Types of compositions:
- Based on antibiotics (2-3 types), used for the treatment of periodontitis. Another component is a corticosteroid, which eliminates inflammation. Validity period: 3-7 days, example: Septomixin.
- Containing metronidazole (“Grinazol”) - antimicrobial agents to eliminate anaerobic flora. Used for periodontitis and pulpitis, they require daily updating.
- With antiseptics (“Tempofor”), they are used for filling the canals of temporary teeth, as well as in adults for the treatment of pulpitis.
- With calcium hydroxide (“Enocal”), which has an osteoplastic and bactericidal effect. Prescribed in the presence of bone destruction. Replace every six weeks until results are achieved.
Materials for canal filling can be hardening or non-hardening.
Pastes containing calcium hydroxide are also used to treat canals due to their sterilizing effect. According to research, the method allows you to achieve sterility at the level of 97% (for example, when treated with saline solution it reaches 20%). It is recommended to fill the canals with such pastes after instrumentation, and after 3 days to place a permanent filling.
Hardening pastes
The materials used to install permanent fillings harden. These include:
- Zinc phosphate cements are used to install fillings in teeth that have one root with a wide canal. They do not change the color of the tooth, do not dissolve, but harden very quickly, so they are used to a limited extent.
- Compositions with zinc and eugenol can have an anti-inflammatory effect and have an optimal hardening time, but can cause allergies and dissolve.
- Pastes based on calcium trioxide have an osteotropic effect, but it lasts until hardening.
- Products with epoxy resins are characterized by heat resistance and the ability to maintain stability. Negative properties - susceptibility to shrinkage, failure of sealing due to insufficient drying of the space inside the root.
- Resocin-formalin materials have an antiseptic effect, but can stain the crown and irritate the periodontium.
- Glass ionomer cements. These pastes are characterized by good adhesiveness, biological compatibility, and high stability. They are difficult to remove when necessary, so they are used together with pins.
The choice of filling material depends on many factors.
One of the promising developments currently at the implementation stage is a product consisting of two calcium compounds. It is characterized by good biological compatibility, tight adherence to the walls, and low solubility.
Pins
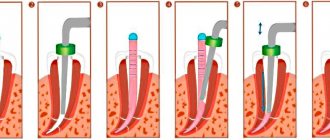
Pins, called primary hard materials, are used in conjunction with sealers - products that fill the space to the walls and provide a tight seal. The most popular types are gutta-percha products. This material fills the canals well, is quickly removed if necessary, is stable, does not irritate tissue, and is radiopaque.
Difficulties may arise due to its softness, so only a qualified dentist should install such pins. Other types of pins are also used:
- Metal , most often titanium or silver. They are used infrequently due to significant disadvantages: they are stronger than dentin, so deformation under the influence of chewing load occurs at different rates, which leads to the appearance of cracks on the crown.
- Fiberglass – new designs used in cases of severe tooth decay. They do not cause allergies, are homogeneous with tissues and are aesthetic, therefore they are used to restore the anterior incisors.
Pins are used in conjunction with sealers.
Temporary filling materials for root canals
Temporary filling of root canals involves filling their lumen with a paste that has a therapeutic effect. Some time after achieving the desired result or after the end of the therapeutic effect, the paste is removed from the canal. Therefore, only non-hardening pastes are used for temporary filling of root canals.
This is quite effective, convenient and allows for more differentiated and predictable treatment of destructive forms of periodontitis, cystogranulomas, radicular cysts and “medicated” periodontitis.
Classification:
.Pastes based on antibiotics and corticosteroids
.Pastes based on metronidazole
.Pastes based on long-acting antiseptics
Pastes based on calcium hydroxide [1]
Pastes based on antibiotics and corticosteroids
Typically, such pastes include two or three antibiotics with a wide range of antibacterial and antifungal effects. Another component of the paste - a corticosteroid, more often - dexamethasone - is used in such a dosage that, while reducing inflammatory and allergic phenomena, it does not affect the protective reactions of the periodontium and the body as a whole. The third component, a radiopaque filler, allows you to objectively assess the quality of filling the canal. These pastes have a strong but short-lived effect; they are introduced into the canal for a period of 3-7 days.
"Septomixine forte" is a non-hardening, absorbable antibacterial paste with a wide spectrum of action. The inclusion of three broad-spectrum antibiotics (polymyxin B sulfate, tyrothricin, neomycin sulfate) makes it possible to effectively suppress the microflora of the root canal, avoiding the formation of antibiotic-resistant strains. The corticosteroid drug dexamethasone in the applied dosage reduces inflammatory and allergic phenomena without affecting the body's defense reactions. A radiopaque filler allows, if necessary, to control the quality of filling the root canal with paste. "Septomixin Forte" is used in the treatment of acute and exacerbations of chronic forms of periodontitis, "arsenic" periodontitis. In this case, the canal, carefully treated mechanically and medicinally, is filled with Septomyxin Forte using a canal filler. For destructive forms of periodontitis, it is recommended to remove the paste beyond the apex. The tooth is covered with an airtight bandage. During repeated visits at intervals of two to ten days, the paste is removed from the canals and replaced with a new portion of Septomixin Forte. With positive dynamics of the pathological process (disappearance of pain and inflammation, cessation of exudation), the canal is cleaned and sealed with a hardening material, for example, Endomethasone. [12]
Pastes based on metronidazole
Megronidazole effectively suppresses the anaerobic microflora of root canals, stops the catabolic destruction of tissue, blocking inflammatory phenomena at the biochemical level. Along with this, practically no allergic reactions or addiction phenomena to this drug have been observed so far.
Metronidazole-based pastes are intended for temporary filling of heavily infected tooth root canals, especially when one can expect a predominance of anaerobic microflora in them (with gangrenous pulpitis, acute and exacerbations of chronic forms of periodontitis). They allow even acute periodontitis to be treated with a hermetically sealed tooth cavity. This prevents secondary infection of the periodontium by oral microflora and improves the prognosis of the disease.
A metronidazole-based paste is injected into the canal using a canal filler, a sterile cotton ball is placed at the mouth of the canal, and the tooth is sealed with a bandage. It should be borne in mind that metronidazole-based pastes are intended for active treatment, so the paste in the canal is changed daily until all symptoms of acute inflammation completely disappear.
The drug "Grinazole" is a paste containing 10% metronidazole. The method of using “Grinazol” has some features.
Firstly, “Grinazol”, having a strong bactericidal effect on the microflora of the canals, allows you to postpone full instrumental treatment of the canal until subsequent visits, when acute inflammatory phenomena subside and this procedure becomes less painful for the patient.
Secondly, “Grinazol” allows even acute and aggravated chronic periodontitis to be treated with a hermetically sealed tooth cavity, i.e. Don't "leave the tooth open." This prevents secondary infection of the periodontium by the microflora of the dental cavity and improves the prognosis of the disease.
Thirdly, “Grinazol” is intended for active treatment; the paste in the canal should be changed daily until all symptoms of the disease completely disappear (pain on percussion, suppuration from the canal, pain on palpation along the transitional fold in the area of the projection of the root apex, etc.) .
Fourthly, “Grinazol”, by changing the environment in the canal and periodontal tissues, allows one to avoid painful phenomena after filling a tooth (“reaction to filling”).
Fifthly, in some cases (presence of general symptoms of inflammation, severe general condition of the patient), along with the local use of Grinazol, general treatment with antibiotics is indicated. [13]
Pastes based on long-acting antiseptics
The composition of drugs in this group usually includes potent antiseptics: thymol, cresol, iodoform, camphor, menthol, etc.
These pastes are radiopaque, do not harden, and slowly dissolve in the canals. They are used for temporary filling of canals in adults during the treatment of pulpitis and periodontitis, during endodontic treatment of baby teeth, including those with absorbable roots (in this case, the paste acts as a permanent filling material).
Tempophore paste consists of a mixture of antiseptics thymol, creosote, iodoform and camphor with the addition of mengol. It is radiopaque, does not harden, and slowly dissolves in the canals. "Tempofor" has a disinfectant and deodorizing effect, does not cause dysbacteriosis, and stimulates the protective properties of periodontal tissues. When used in pediatric dental practice, it does not interfere with the development of the permanent tooth germ.
"Tempofor" allows you to quickly relieve painful manifestations during the treatment of pulpitis, reduce the risk of a painful reaction after filling the canals. This drug is used for temporary canal filling in adults in the treatment of pulpitis and periodontitis, and in the endodontic treatment of baby teeth, including those with absorbable roots. In pediatric dentistry, the use of Tempofor is indicated as a “permanent” filling material for filling the canals of baby teeth.
Calcium hydroxide pastes
Great hopes are currently placed on temporary filling of root canals with non-hardening pastes based on calcium hydroxide. Due to its highly alkaline reaction (pH - about 12), calcium hydroxide, when filling the root canal with it, has a bactericidal effect, destroys necrotic tissue, and stimulates osteo-, dentin- and cementogenesis.
The use of non-hardening pastes based on calcium hydroxide is indicated as a temporary intra-canal medicine in the treatment of destructive forms of periodontitis, cystogranulomas and radicular cysts.
When using these drugs, the canal, carefully treated mechanically and medicinally, is filled with paste using a canal filler. For destructive forms, it is recommended to remove the paste from the top. The tooth is covered with an airtight bandage.
Impassable channels
The listed funds may not always be used. If it is discovered that the canals are impassable, other techniques are used. This situation occurs due to age-related obliteration or due to curvature, inflammatory processes, and also for other reasons. The following treatment methods are practiced:
- Removal of the coronal part of the nerve and mummification of the root. For mummification, a mixture of resocin and formaldehyde is used.
- A similar procedure, but with a silvering , after which the teeth are painted gray.
- Depopheresis. Under the influence of an electric current, copper-calcium hydroxide enters areas of the channels that are inaccessible for mechanical treatment. The ions of the substance accumulate and turn into sediment, which clogs the tubules.
Features of choice
When choosing a paste or pin, the dentist focuses on several criteria :
- Whether the tooth is milky or permanent, what condition its roots are in. During the period of change of temporary units, their roots are absorbed, so the material must have the same ability.
- The shape of the channels and their patency. Metal or fiberglass posts are used if the canals are wide, straight and there is no risk of root damage. It is not recommended to install such models in curved canals, giving preference to gutta-percha products.
- Degree of crown preservation. In case of severe damage, metal or fiberglass pins are used.
- Financial opportunities. The most budget-friendly solution is to fill the canal with cement paste, but it is not always acceptable in terms of the quality and durability of the treatment.
Endodontic treatment is one of the most important areas in dentistry, since its main task is to eliminate diseases of the tooth base and roots. If the material is chosen incorrectly, complications are inevitable - the development of allergic reactions, inflammatory processes, including in bone tissue.
Sources:
- Borovsky E.V. Clinical endodontics. Moscow, 2003.
- Lukinykh A.M. Pulpitis. Tutorial. Nizhny Novgorod, 2005.
- Propaedeutic dentistry, textbook. Ed. E.A. Bazikyan. Moscow, 2008.