Instrumental treatment of root canals of temporary teeth
In this case, specialists do not need to give the cavity being treated a standard cone shape, since this can lead to dangerous thinning of the very fragile walls. The main task in the canal treatment process is to remove infected predentin and create an apical stop. However, reamers are used only when it is necessary to process very narrow cavities. In most cases, H-files are used during the treatment process. The diameter of the instrument increases as it goes deeper into the root canal. There is no standard for the amount of expansion of the internal root cavity. But in practice, the canals of molars are usually increased to 25-35 sizes, and of the front teeth - to 70-90 or more. The main requirement is that the expansion of the cavity should not exceed 2-3 times the size of the original size of the apical section. It is also recommended to correctly prioritize by preparing the more complex mesial and buccal canals of molars first.
Basic principles and techniques of irrigation of the root canal system in endodontics
A.V. Bolyachin, Ph.D., Moscow T.S. Belyaeva, dentist, Moscow
Summary
Analysis of the reasons for the failure of endodontic treatment led to some rethinking of the meaning of its individual stages. Biological prerequisites, such as the complexity of the internal morphology of the tooth, as well as intracanal biofilm, force the search for new effective methods for cleaning root canals. And in this regard, the problem of high-quality root canal irrigation comes to the fore as the key to successful endodontics. The article provides a classification and brief description of the main irrigation techniques in endodontics, and provides practical recommendations for the use of the most popular of them.
Key words: root canal irrigation, ultrasonic and sonic irrigation, hydrodynamic irrigation, photoactivated disinfection, intracanal biofilm.
If we analyze the scientific endodontic literature over the past few years, it becomes quite obvious that in the process of endodontic treatment, the irrigation phase is given great importance. In 2007, JOE (the official publication of the American Endodontic Association) alone published 21 articles on irrigation techniques and irrigant solutions. On the other hand, a colossal amount of research is currently being conducted on rotating NiTi instruments, root canal preparation techniques, and comparison of various systems with each other.
The beginning of the clinical use of NiTi files was accompanied by a certain “euphoria” due to the “virtually unlimited possibilities” of these instruments. Indeed, much of the work indicates a significant difference in the quality of root canal preparations performed with hand instruments and rotating NiTi systems. However, the use of modern research methods such as electron microscopy, microbiological samples, etc. showed that it is not possible to qualitatively clean the root canal system only through mechanical removal of infected dentin and pulp residues with endodontic instruments, whether manual or machine files. (Dalton et al., 1998; Peters, 2001; Nair et al., 2005).
Today, endodontic science has extensive information about the structure of the root canal system. It is known that the internal morphology of the tooth is extremely complex and diverse. A perfectly round cross-section, tapered root canal with a single apical foramen is perhaps the rare exception rather than the rule. In the vast majority of cases, the canals have an irregular shape, different diameters in the buccolingual and mesiodistal directions, and numerous undercuts, the so-called “fins” (Fig. 1, 2). Oval or C-shaped canals are often found. In addition, many lateral tubules arise from the main canal at different levels. Lateral tubules are also found in the area of bifurcations and trifurcations of multi-rooted teeth. There are numerous anastomoses and isthmuses between the root canals, which are especially common, for example, between the mesial canals of mandibular molars. The morphology of the apical third of the root is very complex. It is known that the main canal in the apical part forms a delta and opens at the root apex with not one, but several apical openings. Based on the above, it becomes obvious that such a complex system is not possible to clean only mechanically. In this regard, high-quality and effective irrigation of root canals is of great importance.
Fig.1. The proximal part of the oval canal of the mandibular premolar (the so-called “fin”).
Fig.2. The isthmus connecting the buccal and palatal canals of the maxillary premolar.
Another major problem in root canal disinfection is intracanal biofilm. Its role in the prognosis of endodontic treatment is difficult to overestimate. According to the modern concept, microorganisms in root canals are present in the form of a bacterial biofilm, which significantly changes their properties and makes it difficult to eliminate them from the root canal system. Biofilm is a community of microorganisms surrounded by an extracellular polysaccharide matrix and attached to a moist surface. The biofilm protects the microorganisms present in it from the effects of unfavorable factors, creates favorable conditions for reproduction, the polysaccharide matrix prevents the penetration of antibacterial agents into the biofilm, thereby increasing the resistance of microbes to antiseptics and antibiotics. Therefore, to eliminate biofilm, a combination of both a mechanical factor that can destroy the structure of the biofilm and a disinfectant that destroys its constituent microorganisms is necessary.
Thus, irrigation has two important goals:
- Cleansing the root canal system due to the chemical dissolution of organic and inorganic residues, as well as their mechanical washing out with a stream of liquid;
- Disinfection of the root canal system.
In this regard, cleaning the root canal system should be considered as the most important stage of endodontic treatment, which has a significant impact on its prognosis. In turn, high-quality preparation and formation of the root canal helps create the necessary reservoir for the irrigation solution and opportunities for its activation.
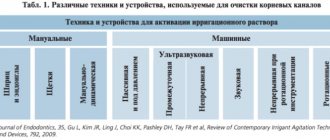
All irrigation techniques can be divided into 5 groups (Van der Sluis, 2007):
- Manual;
- Ultrasonic;
- Sound (EndoActivator);
- Laser (the solution is activated by a laser);
- Hydrodynamic (RinsEndo, EndoVac).
Traditional methods of irrigation using a syringe and endodontic needle provide satisfactory treatment of the coronal and middle third of the root canal, but are not sufficiently effective in cleaning the walls of the apex (O'Connel, 2000). For successful irrigation, it is necessary that the disinfectant solution be delivered to the entire working length of the root canal. This is not always possible to achieve with the help of classic endodontic syringes and needles, since in narrow root canals, due to surface tension, the irrigation solution does not reach the apex, leaving a so-called “air bubble”. As a result, the apical part of the root canal remains insufficiently processed.
There are a number of simple rules and techniques that can make syringe irrigation more effective and predictable.
The effectiveness of this type of irrigation is limited to a distance of 3-4 mm from the needle tip (Sedgley et al., 2005). Consequently, the closer the needle is advanced to the apex, the higher the quality of canal cleaning. On the other hand, the likelihood of the irrigation solution being carried beyond the apex also increases. In order to prevent this complication, it is very important to have some distance between the tip of the needle and the wall of the root canal (Fig. 3a, b).
Fig.3. Movement of the irrigation solution in the root canal: a – in a wide root canal, the solution spreads along the walls towards the mouth of the canal; b – in a narrow root canal there is no space between the canal wall and the tip of the needle and the solution flows into the periapex.
The next important point is the movement of the needle during the introduction of the irrigation solution, as well as the position of the syringe. The irrigant should be withdrawn slowly, carefully, while the needle should make back-and-forth movements. It is recommended to press on the syringe piston with the index finger rather than the thumb, since tactile control is significantly improved (Fig. 4a, b).
Fig.4. The position of the fingers and the syringe when performing manual irrigation: a – correct; b – incorrect.
The depth of needle penetration, in turn, is determined by the following factors:
- The size of the apical preparation.
- Taper of the channel.
- Needle diameter.
The optimal apical preparation size for effective irrigation should be ISO 30, 40 (Hsieh et al., 2007). Schematically, the relationship between apical size and taper can be represented as follows (Fig. 5).
Fig.5. Dependence of the diameter of the root canal at various levels on the taper of the instrument used (explanation in the text).
After completing the preparation of the canal with a hand file No. 25 (taper 2%), it can be assumed that its diameter at a distance of 3 mm from the apex will be 0.31 mm (0.25 + 0.02x3). When using a rotating nickel-titanium file with the same tip size, but a 6% taper, the canal diameter at the same level will already be 0.43 mm (0.25 + 0.06 x3). At a distance of 10 mm from the top, the difference will be even more significant - 0.45 and 0.85 mm, respectively. Thus, the pronounced taper significantly improves the efficiency of irrigation, creating an additional depot for the solution and allowing it to act throughout the entire canal (Fig. 6).
Fig.6. The use of conical root canal instruments increases the efficiency of irrigation by creating a reservoir for the irrigant.
The next important factor is the diameter of the needle. The diameter of needles is usually measured in units called gauge. The most commonly used endodontic needles are 27 gauge. It should be remembered that when determining the size of needles, an inverse relationship is observed. The larger the number in gauge, the smaller the needle diameter (Table 1). Thin needles Endo-Eze Tips and NaviTip (Ultradent) have a diameter of 29 gauge (0.28 mm), which allows you to advance it as far as possible to the apex (Fig. 7).
Fig.7. Irrigation needles NaviTip (Ultradent).
A very important characteristic is the flexibility of the needle and the ability to pre-bend it when working in a canal with pronounced curvature.
Table 1. The ratio of the diameter of endodontic needles in gauge and mm.
| gauge | mm |
| 23 | 0,57 |
| 25 | 0,45 |
| 27 | 0,36 |
| 29 | 0,28 |
| 30 | 0,25 |
To increase the efficiency of manual (performed with a syringe) irrigation, a gutta-percha pin can be used, which mechanically activates the irrigant in the pulp cavity and root canals (Machtou, 1980 (Fig. 8a, b)).
Fig.8. Activation of the irrigant solution using a gutta-percha pin (according to Masht): a – a transparent irrigant solution fills the root canals and pulp chamber; b – turbidity of the solution indicates its activity.
Ultradent offers the NaviTip FX endodontic attachment, which is both a needle and a brush for mechanical activation of the solution. Using NaviTip FX, you can carry out the irrigation and mechanical cleaning of the canal from sawdust and old filling material in one step (Fig. 9, 10).
Fig.9. The endodontic attachment NaviTip FX (Ultradent) is simultaneously a needle for rinsing and a brush for mechanical activation of the irrigant.
Fig. 10. Removing temporary filling material from the root canal using the NaviTip FX attachment (Ultradent).
An effective method of activating the irrigation solution is the use of passive ultrasonation. With passive ultrasonic irrigation, a thin wire or a small file, for example No. 15 or 20, is inserted into the root canal filled with solution (Fig. 11).
Fig. 11. Ultrasonic attachment for passive ultrasonization.
Ultrasonic vibrations and the energy of the file are transferred to the liquid, which causes the occurrence of so-called acoustic cavitation. At the moment of rarefaction, cavitation bubbles appear in an intense sound wave, which collapse sharply when moving to an area of high pressure. In the cavitation region, powerful hydrodynamic micro-shock waves and micro-flows arise. In addition, the collapse of bubbles is accompanied by strong local heating of the liquid and the release of gas. Such exposure leads to the destruction of even such durable substances as steel and quartz. If sodium hypochlorite is used as a solution during passive ultrasonic irrigation, its antibacterial effect is significantly enhanced. In addition, local temperature increases also play an important role. Thanks to these effects, dentinal filings, pulp tissue and intracanal biofilm are removed (including due to the dissolving effect of NaOCl). In order to remove this suspension from the canal, you need 2 ml of fresh solution, which is injected from a syringe.
Practical recommendations for performing ultrasonic irrigation:
- The ultrasound file size should not be more than 15, 20 ISO;
- The files used should not have a cutting surface to prevent transport of the canal (Fig. 12);
- The file should be inserted into the canal 1.5 - 2 mm without reaching the working length (Fig. 13);
- It is important to limit the reciprocating movements of the instrument in the canal and always pre-bend the file when working in curved root canals in order to prevent apical perforation and the formation of steps;
- The solution is sounded 3 times for 20 seconds, with the obligatory renewal of the irrigant in a volume of 1.5 -2 ml.
Fig. 12. Electron diffraction pattern of an ultrasound file for passive ultrasonization. Note the lack of cutting edges and the non-aggressive tip of the tool.
Fig. 13. Methodology for passive ultrasonic irrigation. The file is inserted into the canal 2 mm shorter than the working length.
In addition to ultrasonic energy, sound vibrations are also used to activate the irrigant solution in the root canal. Compared to ultrasonic devices, sound devices generate vibrations of lower frequency but higher amplitude. As a result, the point contact of the sonic tip with the wall of the root canal does not actually affect the efficiency of its operation, unlike ultrasonic tips. The effectiveness of using sound energy for disinfection of root canals has been demonstrated in a number of studies (Walmsley et al., 1989; Jensen et al., 1999; Pitt, 2005; Caron, 2007). An example of a sound system for use in endodontics is the EndoActivator (Advanced Endodontics). An interesting design feature of this system is that it uses special polymer tips that do not have cutting properties and, as a result, avoid complications such as the formation of a step, transportation, and perforation of the root canal walls (Ruddle, 2008). In addition, the tips are disposable and can be easily selected and trimmed depending on the length and diameter of the root canal. On the other hand, RA Sabins and colleagues, comparing the quality of treatment of the apical part of root canals, indicate the advantage of passive ultrasonic irrigation compared to sonic (Sabins, 2003).
To improve the quality of treatment of the apical third of the root, the RinsEndo system (Dürr Dental, Germany) was also developed. RinsEndo is a handpiece that screws onto the turbine drive of the dental unit and uses compressed air pressure to propel the irrigant solution into the apical part of the root canal. A study conducted by V. Hauser and colleagues demonstrated the high efficiency of cleaning the root canal walls using this system compared to traditional manual syringes (Hauser et al., 2007). But at the same time, this work showed that the use of the RinsEndo tip significantly increases the likelihood of the irrigation solution being removed beyond the apex (80% versus 13% when using a conventional syringe), which is especially dangerous when using sodium hypochlorite solution as an irrigant due to the possibility the occurrence of serious complications.
Another option for solving the problem of insufficient cleaning of the apical third of the root canal is the use of systems with simultaneous aspiration of the injected irrigant.
An example of such a system is EndoVac (Discus Dental). The basis of traditional irrigation methods is the passive introduction of an irrigant solution into the root canal under the influence of positive pressure applied to the syringe plunger. The principle of operation of the EndoVac system is based on the movement of the irrigation solution by creating negative pressure in the root canal. One of the nozzles, which supplies the irrigation solution, is inserted into the tooth cavity to a shallow depth, while the other cannula, which performs aspiration, is inserted into the root canal to its entire working length. As a result, the supplied solution, due to negative pressure, penetrates the entire working length of the root canal without the risk of being carried beyond the apex. The advantages of this technique compared to the traditional irrigation method have been confirmed by a number of scientific studies (Fukumoto et al., 2006; Nielson et. al., 2007).
A relatively new and interesting trend in root canal irrigation is photoactivated disinfection (PAD or PDT). The essence of the method is the introduction of a special dye - a photosensitizer - into the root canal, followed by irradiation using low-power laser radiation with a certain wavelength. Light-sensitive dye molecules (most often used for this purpose are tolonium chloride or TBO) attach to the bacterial cell membrane or even penetrate into it. Then, under the influence of laser radiation with a certain wavelength (for tolonium chloride it is 633 nm), a chain of chemical reactions is launched, which results in the formation of free radicals, namely singlet oxygen. These active radicals cause disruption of the integrity of the bacterial cell wall, inactivation of bacterial toxins, degradation of essential proteins and DNA molecules, resulting in the death of the bacterial cell (Lambrechts et al., 2006). The high antibacterial activity of PAD against both suspended cultures and bacterial biofilm has been demonstrated in a number of studies (Bonsor et.al., 2006; Williams et al., 2006; Soukos et al., 2006). The key point of this technique is the direct contact of photosensitizer molecules with the bacterial cell and its penetration into the bacterial biofilm. Consequently, as in the case of the use of traditional irrigation methods, the problem of delivering irrigant (dye) to hard-to-reach corners of the root canal system remains relevant. To activate the photosensitizer solution, all the methods described above are applicable.
In conclusion, I would like to note once again that today the endodontic treatment strategy is increasingly inclined to use the concept of the biological feasibility of the intervention. This approach, in turn, led to the need to improve methods of combating intracanal biofilm, as the main reason for the failure of endodontic treatment. And the key point in this fight is high-quality irrigation of the root canal system.
Treatment of permanent teeth at the stage of root canal formation
In this case, instrumental preparation is carried out similarly to the previous option. The specialist cleans the walls of the root canals with large H-files that have a safe tip. As in the treatment of temporary teeth, the internal cavity does not need to be given a conical shape, since at the stage of active formation the dentin layer remains very thin. In the process of removing infected tissue, the dentist needs to guide the instrument in such a way as to ensure the highest quality cleaning of the root canal, which expands towards the top.
Instrumental treatment of formed dental root canals
Endodontic treatment of permanent teeth that already have a fully developed root canal system is carried out using methods used for adult patients. During the treatment process, the doctor’s main tasks are to give the cavity a funnel shape with minimal expansion in the area of physiological narrowing and maximum expansion at the entrance. The specialist also needs to ensure that the position of the apical foramen remains unchanged and form a reliable stop for the filling material. During the instrumental treatment of permanent teeth, it is recommended to regularly rinse the cavity. K-reamers, as well as H- and K-files can be used to scrape tissue from the canal walls. The preparation technique can be based on one of the following methods:
- Step-back. Also known as the apical-coronal technique or “step back”. Involves the expansion of root canals from the apical foramen towards the orifices. Requires the use of tools with ever increasing diameter sizes.
- Step-down. This technique is also called “step forward” or coronal-apical. In this case, canal processing is performed in the opposite direction to the previous method: from the root orifices to the apex.
- Combined. This hybrid method involves the use of two techniques at once. As a rule, at the initial stage, the crown is processed using the step-back principle, after which the canals are developed using the step-down method.
PREPARATION OF THE ROOT CAVITY OF THE TOOTH
Preparation of the root cavity of a tooth involves removing soft tissue and infected dentin from the canal and giving it a uniformly tapering conical shape.
During instrumental processing, 15-50 microns of tissue are removed from the root canal wall (the average thickness of infected dentin). Some sources indicate the need to expand the canal by at least three instrument sizes, and much more when working in infected canals. Requirements for preparation of the root cavity of a tooth: 1. Creation of a funnel-shaped canal with a minimum diameter in the area of the physiological opening and a maximum at its entrance; the shape of the prepared canal should exactly repeat its original shape (not deform the canal), but be larger in diameter. 2. Maintaining a balance between the diameter of the channel and the thickness of its walls. 3. Maintaining the same position of the apical foramen. 4. Creation of a holding form for the filling material. 5. Creating sufficient resistance at the apical foramen (apical stop), preventing the filling material from being pushed into the periodontium. 6. Permanent cavity toilet. When instrumenting the root canal, the most common mistakes should be avoided, such as the formation of steps that contribute to the accumulation of sawdust in the canal, funnel-shaped expansion of the apical foramen and the creation of “knees” when using sharp hard instruments, perforation along the minor curvature of the canal, where maximum dentin removal is usually carried out. A blower should not be used in the canal (to prevent embolism). When working in root canals, the following techniques are usually used: 1. R i m i n g - work with reamers and K-files, including sequential insertion of the instrument into the canal, its rotation and withdrawal. The most common complication of rimming is instrument fracture. 2. F i l i n g - work using K- and N-files, including scraping tissue from the walls of the canal with vertical up and down movements without rotation. A complication is the formation of steps and a change in the shape of the canal due to the effect of straightening the instrument. In the specialized literature, the first file that reaches the apex is called initial apical file (IAF), the last file that reaches the apex and forms the “apical stop” is called apical master file (AMF), the last (largest diameter) file that processes the canal is final file(FF). All currently existing methods of root canal preparation are based on one of two techniques called step-back ("step back" - expansion of the canal from the apical foramen to the mouth using instruments of increasing diameter), step-down ("step forward" - development of the canal in the direction from the mouth to the apex) or are a combination of these techniques. Step-back technique (“step back”) Conditions necessary for the implementation of the technique 1. Use of pre-bent instruments in curved canals (bending is carried out in accordance with X-ray data and taking into account the working length of the instrument). 2. Treat the instrument before insertion into the canal with special lubricants (lubricants - Gly-Oxide, File-Eze, KY Jelly or liquid soap). Lubricating agents, reducing the resistance of the surface of the canal walls, facilitate the advancement of the instrument, help the rinsing solutions reach the apex, and emulsify the tissue in the canal, thereby facilitating its removal using the instrument. Some lubricants contain EDTA [Canal+ (Septodont), HPU 15 (Spad), RC-prep (Premier)] 3. Use of the “Watch-Winding” technique, according to which, after the tool reaches its working depth in the canal is rotated 2-3 times clockwise and counterclockwise by a quarter turn, followed by retraction. Sometimes short, light “pushes” of the instrument into the canal to a depth of up to 1 mm are allowed. 4. After removal of the instruments, each of them should be cleaned, re-bent (if necessary) and treated with a lubricant. 5. Constant (after each movement of the instrument) irrigation of the canal. Processing technique. First, a prepared thin (08-10 size) K-file is inserted into the canal for the entire working length of the tooth, determined earlier and marked on the instrument with a limiter. Work with a tool of this size continues until it passes through the canal completely freely. Then the same procedure is carried out with a file of the next size. After achieving free movement in the canal of this file, a control passage of the canal with the previous (smaller) instrument size is carried out (to prevent blocking of the apical hole with sawdust). In this way, the canal is expanded over the entire length to at least 25 instrument sizes (the minimum file size that provides sufficient for good cleaning and obturation of the root canal. The approximate sequence of sizes of instruments used: 10-15-10-20-15-25-20. After After completing the processing of the apical part with instrument 25, instrument 30 is inserted into the canal, the working length of which is 1 mm less than the last apical file. After completion of the work with this instrument, it is necessary to carry out the so-called recapitulation - control processing with the last apical file (25) to smooth out the formed steps and prevent clogging of the canal dentine filings. After file 30, use size 35, the working length of which is 2 mm less than the working length of the tooth, then 40 by 3 mm, etc. (Fig. 48). After using an instrument of each size, it is necessary to perform recapitulation, for which you can also use the H-file (Fig. 48).The coronal and ostial thirds of the canal can be processed using Gates-Glidden burs or orifice expanders (Fig. 50). After completing the work, a sodium hypochlorite solution is injected into the apical third and left there for 5-10 minutes to clean additional tubules. In thin, curved or petrified canals, it is possible to use EDTA, which dissolves and washes out mineral salts. For this purpose, EDTA can be used as a lubricant for A-file08. In the apical area, it is possible to create a retention zone for the pin by forming parallel walls over a distance of 3 mm from the physiological narrowing of the canal.
Step-down or crown down technique (“step forward” or “from the crown down”)
The advantages of the method are minimal pushing of debris beyond the apex, creating better access and control of the apex, reducing the risk of widening the apical foramen, and creating a sufficient path for irrigation. The method is effective in difficult-to-pass channels. The working length of the canal is determined not before its treatment, but after providing access to the apical third. Processing technique. The mouth of the canal is filled with sodium hypochlorite, after which “npe-Gates preparation” is carried out: file 35 is inserted into the canal until it stops and its length is fixed. If a file of this size cannot be entered, enter a smaller one. The file is processed until it moves freely in the canal to a fixed length. Then the same length is treated with Gates-Glidden burs No. 1 and 2 (up to bur size 80). After this, file 30 is inserted into the canal until it stops, its length is fixed, and a section of the canal is developed. Then the treatment is carried out to the achievable (all the way) length with a file of 25 and then smaller ones - until the working length of the canal is reached. When the expected working length is reached, its exact determination is carried out. After this, the apical part is gradually expanded to file 25. The walls are leveled with H-files 30-35.
Hybrid technique (step-down + step-back) Treatment of the root canal begins with expansion of its coronal third using Gates-Glidden burs from sizes 1 to 6. If insertion of a Gates-Glidden size 1 bur is not possible, the work should be done with files. The Gates-Glidden 3 bur is inserted at 1/2 the length developed by the Gates-Glidden 1 and 2 burs, Gates-Glidden 4, 5 and b work only at the mouth. After this, the canal is developed using the step-back technique to a distance of 1 mm from the prepared part. The walls are aligned using an H-file.
Features of machine treatment of dental canals in children
Regardless of the technique used, the dental specialist should consider the following points:
- Curved canals should be treated with a pre-curved tool.
- After removal, the reamers and files need to be cleaned and checked for damage.
- Rinsing the treated area should be done using an endodontic syringe equipped with a special needle.
Particular attention should be paid to medicinal treatment of the canals using EDTA and other drugs. It should be carried out at all stages of instrumental preparation, from the initial opening of the cavity to the final washing out before filling.
Canal treatment
Why are channels so important? Why is it necessary to treat dental canals?
The root of a tooth is a system of branched channels through which useful substances flow and innervation of the tooth is ensured. Damage to the tissues that form these canals and the lack of timely and high-quality treatment will certainly lead to tooth loss. At the same time, the complexity of root canal treatment is evidenced by the fact that the number of roots in a tooth varies, they can have bends and branches.
To carry out endodontic therapy at the highest level, it is necessary to combine high professionalism of specialists, excellent equipment of the dental center, and the use of only high-quality materials.
The Dentist clinic fully complies with all these conditions. IMPORTANT:
To provide high-quality endodontic therapy, it is necessary to have an idea of how many roots the teeth have and what the bends of these roots are.
Materials for canal filling.
The main task that a specialist faces after completing the mechanical and
medicinal treatment of the canal - hermetically seal it. The best result is achieved:
- using the lateral condensation method, which involves the use of gutta-percha pins compacted and fastened together with a cementing substance;
- using the Thermafil system. In this case, gutta-percha heated to 200 degrees under pressure is injected into the canal, which allows you to thoroughly fill all branches and achieve perfect tightness.
- using high-quality antiseptic pastes and cements.
The specialists of the Dentist clinic, striving to perform canal filling with the highest quality possible, use precisely these, the most modern, techniques in their work.
IMPORTANT:
The essence of any canal filling is that the substance introduced after removal of the nerve, mechanical and medicinal treatment of the canal must completely clog the canal to prevent the development of infection in the canal.
Why is mechanical treatment of the canal necessary?
In addition to canal sealing, an equally important part of endodontic treatment is mechanical
canal treatment and sterilization. Experts believe that the persistence of tooth pain after completion of all therapeutic measures, the development of a granuloma or cyst at the apex of the tooth root is due precisely to insufficiently effective actions at this stage. To eliminate the need for tooth extraction due to poor quality treatment, you should entrust the procedure to professionals.
IMPORTANT:
In pursuit of a lower price, during endodontic treatment, patients forget a simple rule: “He who is treated for nothing, is treated for nothing!”
And as a result of this approach, removal followed by implantation
! Although high-quality endodontic treatment would cost much less! But this thought comes to me, it’s too late!
What tools are used?
Treatment of canals is complicated by the fact that narrow convoluted tubules are difficult to treat with medication, and there are difficulties with filling them. Modern clinics, such as Dentist, have the necessary equipment to effectively and efficiently carry out this volume of work. With the use of a multi-functional endodontic handpiece and nickel-titanium instruments, the process has been greatly simplified. Thanks to their sufficient hardness and elasticity, it is possible not only to expand, but also to straighten the tortuous channels. IMPORTANT:
With the advent of the multifunctional endodontic handpiece and
Nickel-titanium instruments, impassable and narrow channels are a thing of the past!
Specialists at the Dentist clinic widely use Japanese endomotors with a built-in apex locator.
With its help, it is possible to achieve unique precision in canal treatment. At the same time, careful execution of all manipulations is guaranteed by triggering the auto-reverse. The presence of a liquid crystal display makes it possible to receive all the necessary information about the channel and fully control the progress of treatment. Endoscopic root canal treatment
is another technology that is used both as a preoperative examination and for active endodontic treatment. With the advent of the endoscope, it is possible to achieve more meaningful monitoring of the working field than with the help of micromirrors and microprobes.
IMPORTANT:
No amount of equipment, even the best, can replace the good hands of a doctor. But such equipment helps the doctor do his job efficiently and with maximum benefit for the patient.
What methods are used?
Two methods are used for endodontic treatment:
instrumental processing of channels. The Step-back technique is a classic option. It involves expanding the canal, starting from the apex, by using instruments from smaller to larger sizes. Root canal treatment from top to bottom, using the Crown Down technique, is a more progressive and safer technique that provides better access to the apex. In this case, the expansion of the root canal proceeds from the mouth to the apex using instruments from larger to smaller sizes. However, to use this technique you need modern equipment, an endomotor. Using this innovative toolkit, the specialists of the Dentist clinic are ready to carry out the entire course of endodontic treatment at a completely new level, ensure a high-quality result, and completely eliminate the development of complications.
Disinfection and sterilization of the canal.
The most modern methods of disinfection and sterilization of tooth canals are international medicinal protocols for canal treatment, the use of a diode laser and the Depophoresis technique.
Laser exposure
provides a bactericidal, anti-inflammatory, immunostimulating effect.
Conducted Depophoresis
, based on the disinfecting properties of copper-calcium hydroxide in an electric field, promotes the restoration of destroyed bone tissue, protects the tooth root from the action of an infectious pathogen.
The cost of root canal treatment near the Chistye Prudy metro station.
The price of root canal treatment in Moscow varies significantly. Moreover, it depends not only on
their quantities. a significant impact on how much root canal treatment costs . The use of optical technology, which provides the best overview of the procedure, also increases costs. Since endodontic treatment at the Dentist clinic is carried out using the most modern equipment, technologies and materials, you should not expect that it will be cheap. Our specialists aim to significantly extend the life of the tooth, and this approach also requires financial costs.
IMPORTANT:
The key to successful endodontic treatment lies in competent medical tactics and high technical equipment of the dental office. It is these components that we are ready to offer you in our clinic!