Filling is the final and most important stage of root canal treatment. If it is carried out incorrectly, complications will inevitably develop immediately or over time. Because of them, you will have to undergo expensive treatment, or even remove the tooth altogether.
Most dentists fill root canals using improper technology. Most often, such cases occur in public clinics. How to avoid such situations, what to pay attention to before and during therapy, what treatment methods to choose and how the patient can control the manipulation is described in the review.
What is root canal obturation?
Obturation is the scientific name for filling. By it we mean the complete filling of the channels with sealing masses. The procedure is needed to strengthen the roots, eliminate the voids formed after depulpation (removal of the pulp - nerve) and, thereby, protect the tooth cavity from the penetration of aggressive substances, pathogenic microorganisms and subsequent inflammation.
Sealants in canals are called root fillings.
Preventing infectious processes is the main goal of filling. To prevent them from developing, the canals must be obturated to the root apex (apex), without bringing the filling material into the periapical space.
Obturation is the scientific name for filling
Unfortunately, bad fillings are common - in 60-70% of cases (according to the medical portal “24Stoma” https://24stoma.ru/plombirovanie-kanalov.html). It appears as a result of poor mechanical and medicinal treatment of the cavity, incorrect measurement of their length, the use of an inappropriate obturation method or cheap materials.
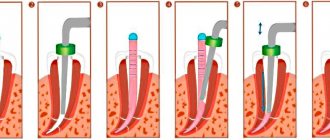
Method using the E&Q Plus system
The E&Q Plus system is a special injection gun with a tip and various attachments. Thanks to it, gutta-percha can be heated to the desired temperature in the root canal itself. Thus, a gradual and constant compaction of the material occurs. The result is a three-dimensional filling.
You can also complete the process using a gun, or by resorting to the vertical condensation method. The filling method using the E&Q Plus system is recognized by dentists as one of the best today. Therefore, it is used most often.
Filling a tooth canal, root canal, what methods exist?
A root filling is placed in one of 5 ways:
- one paste is an outdated technique, which in 90% of cases leads to complications;
- one pin - also considered obsolete, but is actively used in dentistry (mostly budget) due to ease of implementation, good obturation and lower risk of negative consequences;
- lateral condensation is the most common method, relatively easy to use and gives good results;
- vertical condensation - an improved version of the previous type, a more labor-intensive, complex and expensive method;
- injection - is the best, allows you to tightly obstruct the main channels, branches and microtubules.
There are 5 ways to fill canals
Sometimes doctors combine several filling methods. Thus, one of the tooth canals with good patency can be closed using the mono-pin method. The other, curved, using a system with thermoplasticized gutta-percha.
And for the third, excessively wide one, gutta-percha filling will be applied - lateral condensation or vertical compaction.
One paste method
With this method, one sealer is introduced, which hardens on its own. The paste is placed using manual files (notched needles) or automatic endomotors that rotate the files at high speeds (120-800 rpm).
The one-paste method is an outdated and unreliable method of filling. It almost always causes complications.
The technique has other disadvantages:
- uneven distribution of filling material with the formation of voids;
- over time, the pastes shrink and dissolve;
- only the main channel is filled, and the branches and microtubules remain unsealed;
- there is a high risk of the sealer being carried beyond the apex, because It is impossible to fully control the obturation process.
The only advantages of this method are ease of use and bactericidal effect. However, these advantages pale in comparison to the disadvantages.
The one-paste method is outdated and unreliable
Single pin method
The single pin method (also center pin or mono pin) is a compromise between quality and simplicity. It is better than the previous method, gives many fewer complications and obstructs the root canals quite well.
The essence of the technique is to insert one (central) gutta-percha pin onto the sealer. After applying the paste, a conical rod is placed into the canal, which pushes the filling material towards the walls and promotes its uniform distribution.
With this technique, it is possible to slightly fill the apical branches from the main canal with filling material. Due to the pressure created by the pin during insertion, the sealer penetrates into the microtubules.
The monopost method is mainly used in public dentistry. It is simple and inexpensive.
Private clinics prefer other methods of installing root fillings. When filling on a central conical shaft, the material is often pushed beyond the apex. A slight removal of a high-quality, bioinert sealer in most cases does not have consequences, only occasionally pain is possible when biting.
However, if a lot of filling material with necrotizing properties has penetrated into the apical space, inflammation will inevitably develop over time and it will be necessary to resort to resection of the root apex or tooth extraction.
Canal filling using lateral condensation method
The lateral condensation or compaction method is used most often. It is relatively simple and inexpensive. And the effectiveness of obturation is many times higher than when installing root fillings using the single-paste or single-pin method.
Mechanism of filling with lateral compaction:
- the canal cavity is filled with sealer;
- select the main rod (master pin), whose size most accurately matches the length and width of the canal;
- the central rod is inserted;
- then push the master pin against the wall using a spreader - a special compacting tool;
- Several smaller pins are sequentially inserted, each of them is compacted with a spreader;
- in total, 5-12 conical rods are placed in one canal - in the photograph such a root filling looks like a bouquet of stems;
- then an x-ray is taken to determine how well the canal is obturated - if unsuccessful, all pins are removed and lateral condensation is performed again;
- when the canal is tightly sealed without removing the material beyond the apex, the protruding tops of the pins are cut off with a hot tool.
Such a multicomponent root filling makes it possible to tightly obturate the root canal due to the individual selection of gutta-percha rods of various widths and lengths.
The lateral condensation method is most often used.
However, lateral compaction has significant disadvantages:
- during obturation, strong pressure is created on the walls of the canals, which can lead to perforation or fracture;
- the lower third of the canal is closed with only one master pin on the sealer - due to this, it is impossible to tightly seal the apical part.
And yet, the method of lateral condensation of gutta-percha, due to its convenience, simplicity and low cost, is considered the best for endodontic dental treatment.
Vertical condensation of gutta-percha
This method involves obturation of the canals with preheated gutta-percha. There are many variations of the method, but the classic one is carried out in the following sequence of actions:
- select a master pin that matches the size and taper of the canal;
- shorten the central pin by 0.5-1 mm - this is necessary so that when inserted, the rod does not go beyond the root apex;
- they fit the pin in the canal and take an x-ray photo - this is how they check the correct fit of the rod;
- the master pin is softened, inserted into the canal and compacted with hot instruments that keep the gutta-percha warm until it is completely compacted;
- after obturation of the lower third of the canal, condensation is carried out first in the middle and then in the upper part - for this, hot gutta-percha is injected with a special syringe.
The method is labor-intensive, complex and expensive. However, with its help it is possible to almost perfectly obstruct the root canals, all branches and microtubules.
Injection methods
Injection techniques involve injecting heated liquid gutta-percha into the root canals. These techniques exclude the use of a sealer: obturation is achieved only by molten gutta-percha.
High temperature methods are carried out in two ways:
- Liquid gutta-percha is administered using special syringe systems (for example, the Obtura system). It is heated to 160-200°C, after which it is placed into the canal using a cannula (injection needle).
- Softened, but not hot, gutta-percha is injected on a plastic pin using special systems (Ultrafil, Thermafil, Thermafil-Plus). The conical rod is heated in a dental oven until the gutta-percha softens, then it is placed in the canal, and the protruding parts are cut off.
Filling with thermoplastic gutta-percha is considered the best. The molten filling material penetrates into all branches from the main channel and microchannels, seals the cavities hermetically and tightly, and is tightly fixed to the walls.
However, it is worth considering the disadvantages:
- as with any method of placing root fillings, the risk of pushing the material past the apex remains;
- there is a possibility of tissue burns from molten gutta-percha - this is more common when using Obtura and similar systems;
- the question of the reliability of canal obturation without a sealer remains open - gutta-percha is not so reliably fixed in relation to the walls and does not have antibacterial properties;
- high price - if the canal is filled with the Thermofil system or a similar system, on average you will have to pay 2,200 rubles, and the price does not include development, mechanical and medicinal cleaning.
This is a dental microscope.
High-quality filling can be carried out using a cheaper technique - lateral condensation.
However, if the patient’s canals are curved, difficult to navigate, with numerous branches and dead ends, the use of thermoplasticized gutta-percha is the only reliable method of obturation.
Advantages and disadvantages of the method
The liquid gutta-percha technique when performing the protocol ensures the penetration of gutta-percha and sealer into both the main root canal and the dentinal tubules. The effective use of this technique, however, is determined by the doctor's skills, developed and honed on training teeth. The increase in temperature on the outer surface of the root is insignificant and has minimal damaging effects on the tissue.
A conditional disadvantage of this technique is that there is a possibility of gutta-percha and sealer being removed beyond the apical foramen and damaging the periodontium.
The introduction of liquid gutta-percha technique into practice requires additional material costs and is not popular among patients due to its higher cost.
However, although with the conscientious, qualified work of a dentist, even using less expensive techniques and materials, for example, the lateral condensation method of gutta-percha, quite acceptable results can be achieved, the injection gutta-percha method is the most advanced and provides the best results at the moment.
Temporary filling of root canals
Permanent obturation of the root canals immediately after cleaning is possible only when treating pulpitis without purulent processes. In other cases, preliminary temporary filling with calcium hydroxide-based sealers is indicated.
Temporary obturation is used for:
- granulomas and cysts;
- periodontitis;
- pulpitis with a purulent course: chronic ulcerative and hyperplastic, acute gangrenous and accompanied by pulp necrosis;
- perforations.
Temporary filling of root canals is carried out using two methods:
- Hand tools. The length of the root canal is measured and recorded on a file. The tip of the instrument is used to scoop up the paste, which is then injected into the cavity and condensed with a damp piece of cotton wool. Then a second portion of sealer is placed, inserting the needle two-thirds of the length of the canal, followed by a third, inserting the file one-third of the length.
- Using an endocanal micromotor. Take a tool one size smaller than the file used to expand the canal. The canal filler is fixed on the head of the device, immersed in the paste, and then inserted into the canal to the top. Turn it on at low speed (100-120 rpm) for a few seconds, then slowly remove it. Repeat the procedure, immersing the tip of the needle 2/3 of the length of the canal.
After obturation with calcium-containing pastes, the tooth cavity is closed with a temporary filling for 2 days. If pain persists, the procedure is repeated.
Permanent filling of root canals immediately after cleaning is possible in the treatment of pulpitis without purulent processes
How is filling done?
Note that today in dental clinics there are the following methods of filling root canals:
- Using a homogeneous paste, to obtain which a special powder and liquid are mixed. Filling the root canals in this case involves filling the cavity with the resulting pasty material. This composition is used when there are strongly curved and narrow tooth canals.
- Single pin method.
- Lateral condensation method.
- Using the Thermofil system.
- Depophoresis method.
- Using hot gutta-percha.
- Using the E&Q Plus system.
All methods, except the first, involve the use of solid filling materials and/or pins. The use of one or another treatment method depends not so much on the financial capabilities of the patient, but on the anatomical features of his teeth.
Filling methods differ not only in the method of filling the root canal cavity, but also in the speed of the procedure, the durability of the result, and also the cost. Let's consider each method separately.
Filling canals for periodontitis and other purulent processes
With the development of serous inflammatory processes, cleaning and disinfection of the canals alone is not enough. Pathogenic microorganisms penetrate into deep, hard-to-reach areas where they form a film.
If all main canals and their branches are not completely sanitized, re-infection will inevitably develop. To avoid this, in case of purulent pulpitis, periodontitis and granulomas, temporary filling is used.
The following algorithm is used:
- after passing and cleaning the canals, they are treated with a 2% chlorhexidine solution for 2-3 minutes;
- obstruct the canals with a paste containing calcium hydroxide: to enhance the bacteriostatic effect, select sealers that, in addition to hydroxide, contain iodoform, paramonochlorophenol, glycerin, chlorhexidine;
- The paste is left for 2-3 days under a temporary filling, after which the canal is cleaned again and finally obturated.
The use of calcium hydroxide in conjunction with antiseptic drugs helps destroy bacteria and microbes, and also initiates reparative processes. This manipulation reduces the possibility of re-infection and complications by 5-25% (according to information from the professional dental online magazine “Dental Magazine” - https://dentalmagazine.ru/posts/vremennoe-plombirovanie-kornevyx-kanalov-v-sxeme-endodonticheskogo- lecheniya.html).
Gutta-percha points
What is root canal filling?
If endodontic treatment is of poor quality, the canals will have to be unsealed (disobturated) and sealed again. This process is called refilling.
It is prescribed if:
- the sealer has dissolved;
- the filling material was brought beyond the apex;
- the pulp was not completely removed;
- the canals were not hermetically sealed;
- the root canals were not obturated to the apex;
- Secondary inflammation has developed - periodontitis, granuloma, cyst.
The purpose of disobturation is to remove the old filling material and carry out subsequent sanitation and filling of the canals. You can remove the root filling in 2 ways:
- Using drugs (solvents) that soften the sealer. They are applied for a few minutes (if the canals were previously filled with gutta-percha and ordinary pastes) or left for 2-3 days (in teeth obturated with resorcinol-formalin or cement). Afterwards, the remaining filling materials are removed using files and reamers: they are gradually rotated in the canal, each time advancing the needle tip by 2-3 mm.
- Ultrasonic installations. For this I use ultrasonic endodontic motors. Ultrasound destroys the sealer, and files rotating at high speeds clean the canal cavity from paste residues.
Unsealing is a complex process. Dentists do not like to do it and, as a rule, do not provide guarantees for the treatment of such teeth. The chances of success are higher if endodontic therapy is carried out using endomotors and under a dental microscope.
If endodontic treatment is of poor quality, the canals will have to be unfilled.
The latter displays an image of the root canals enlarged up to 30 times, which allows you to examine all the anatomical features and carry out desobturation with microscopic precision.
Lateral condensation of gutta-percha points: stages of filling
The procedure for dental canal filling with gutta-percha pins is performed in several key stages:
- Preliminary preparation of the tooth for filling
All affected tissue is removed and a suitable dental canal cavity is formed. It is washed with a stream of clean water and dried. The cavity is treated with antiseptic agents. - Lateral condensation is performed
The dentist selects a master pin suitable for the canal - it must match the size of the endodontic instrument used to finish the root canal. The selected pin, in its length, should be 1 millimeter shorter than the entire length of the canal - this will ensure reliable, even filling of the upper part of the tooth. The selection of the length of the pin can occur in three different ways: visual (the least reliable), tactile and using x-rays (the most reliable).
- Selecting a side seal
The sprender (dental instrument) is selected so that its length is 1-2 millimeters less than the working length of the dental canal and the master pin;
- Filling a dental canal with paste
The dentist fills the previously prepared root canal with endosealant (special filling paste). The paste should be evenly distributed along the walls of the canal, up to the apical opening, but the canal itself is not completely filled.
- Obturation of the canal with gutta-percha
A pre-prepared pin is installed into the canal (it is pre-coated with filling material). There should be no cavities or air bubbles left in the root canal. To improve the quality of filling, the pin is installed using rotational movements.
- Compaction with spreader
The instrument is inserted into the filling canal using rotational movements - this helps fix the pin to the canal walls. Remains of filling paste are also removed;
- Installing a temporary filling
It is performed if the dentist is not sure about the quality of the filling and wants to check the condition of the canal within 1-3 days after the procedure. As a rule, a temporary filling is installed on teeth with complex root canals.
- Installation of a permanent filling
It is the final stage of gutta-percha filling. Performed in the absence of any problems or complications. Depending on the dentist’s recommendations and the patient’s wishes, various filling materials can be used, including composite and polymer.
Complications after root canal filling
With any obturation method there is a possibility of complications. Among them:
- Inflammatory processes. They occur if the length of the canal was measured incorrectly and it was not completely sealed, due to the lack of antibacterial properties of gutta-percha pins or leaky obturation. Pathogenic microorganisms penetrate into cavities, where they multiply and lead to the formation of periodontitis, granulomas, and cysts.
- Perforations. Appear when there is excessive pressure on the channel during processing. The instrument seems to move to the side, and a hole is formed in the canal wall or at the bottom of the cavity. It urgently needs to be closed with a special material (MTA), otherwise the tooth will have to be removed.
- Pain when biting and neurology. Characteristic of teeth in which the filling material is extended beyond the apex.
- Tool breakage in the canal. The tip of a file, reamer, channel filler, paper file for drying, etc. may remain in the cavity. The doctor must carefully inspect each instrument removed and, if a breakage is detected, immediately inform the patient and carry out appropriate endodontic treatment. If this is not done, inflammation and tooth extraction cannot be avoided in the near future.
The risk of complications and their type depends on the obturation method. So:
- when filling with a single paste or single pin method, periodontitis, cysts and granulomas are often observed;
- filling canals using the method of lateral condensation or vertical compaction reduces the risk of inflammatory processes to a minimum - up to 20%;
- During therapy with the Thermafil system and other similar installations, periodontal burns, post-filling pain, and the formation of granulomas and cysts are likely.
A common medical error is the breaking off of an instrument in the canal.