Causes of obstruction of dental canals
The root canals of teeth can become obstructed for a variety of reasons. The most common include:
- features of the anatomical structure of the tooth - highly curved roots with small branches, flattened areas and transverse bridges;
- inflammatory processes in the neurovascular bundle - with dental injuries and chronic pulpitis with a subacute course, the root canals can become overgrown;
- age-related changes in tissues - over time, dentin deposits accumulate on the walls of the root canals, which lead to a narrowing of the lumen;
- dental procedures using phosphate cement - this material has a high density and cannot be destroyed by ultrasonic waves, instruments and solvents.
Before starting endodontic treatment, it is important to accurately determine whether the canals are patent.
What are channels?
Each tooth has a certain number of roots located under the gum.
How many roots do teeth have? The answer to this question depends on several factors - the position of the unit, the person’s age, heredity, even race. It is known that Mongoloids have more roots than Caucasians.
The standard quantity is as follows:
- Incisors, canines – 1.
- Premolars – 1-3.
- Upper molars – 3-4.
- Lower molars – 2.
- Third molars – 3-5.
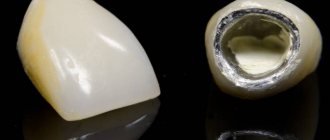
Inside the crown is the pulp, a tissue consisting of blood vessels and nerve endings. They pass into the pulp through the apical foramen, located at the apex of the root, and through canals, narrow cavities inside the root. Their number is not always equal to the number of roots.
The photo shows the beginning of the root canals.
Diagnostics
Treatment of impassable root canals begins with determining their length and anatomical features. The most informative diagnostic method is radiography. To obtain accurate data on the condition of the tissues, a photograph of the tooth root is taken with the instrument inserted into it. This allows you to see:
- length of root canals,
- the presence of curvatures and perforations,
- impassable areas.
The condition of the periodontium is also assessed. This allows you to determine further treatment tactics.
How many canals are there in a tooth?
The configurations of cavities in the roots vary. There are several varieties of them. A dental root may have two apical foramina, branches inside converging to one foramen, or two internal cavities running parallel. The percentage of possible combinations is shown in the table.
| Unit | Quantity |
| Upper incisors, canines | 1 |
| Lower central incisors | 1 (70%) or 2 (30%) |
| Lateral lower incisors | 1-2 (50% each) |
| Lower canines | 2 |
| Upper first premolar | 2 (90%) or 1, 3 (5% each) |
| Lower first premolar | 1-2 |
| Upper second premolar | 2 (90%) or 1, 3 (5% each) |
| Lower second premolar | 1 |
| Upper first molar | 3 or 4 (50% each) |
| Lower first molar | 3 (60%) or 2.4 |
| Upper second molar | 3 (70%) or 4 (30%) |
| Lower second molar | 3 (70%) or 4 (30%) |
| Upper third molar | up to 5 |
| Lower third molar | no more than 3 |
When treating pulpitis, the root canals are cleaned and filled.
Knowing the structure and location of the canals is important for the treatment of pulpitis. When the pulp is inflamed, the root cavities must be cleaned, so before starting treatment, the doctor must have a clear idea of how many there are and what they look like. This information can only be obtained using an x-ray.
The structural features of the canals cause treatment difficulties. A number of problems often arise:
- the cavity is impassable for instruments (curved, branched);
- microorganisms that are particularly resistant to the action of standard antiseptics accumulate in the intraroot spaces;
- bacteria tend to re-enter through the dentinal tubules;
To overcome these problems, dentists use modern equipment and materials - endodontic motors designed for mechanical processing, fillings with strong antiseptics.
Features of treatment
Various techniques are used to treat impassable root canals:
- devital amputation of the pulp followed by mummification,
- depophoresis.
A special approach is required if the root canal:
- strongly curved
- completely closed,
- narrowed,
- is located next to the neighboring root.
To make the canal passable along its entire length, modern dentistry uses:
- durable extractors - nickel-titanium files, which allow you to go through the canal without preliminary tooth preparation;
- drills - special instruments with spiral blades designed for quick and safe removal of gutta-percha, pastes, cements and other filling materials;
- solvents - necessary for unsealing previously sealed canals; they cope well with soft and plastic materials.
The treatment tactics for impassable root canals in each clinical case are determined by the doctor. The procedure is performed under anesthesia. Depending on the complexity, treatment is carried out in one or several stages. To obtain the desired result, 2-3 visits to the dentist may be required.
Solving problems with very curved channels
The ultimate goal of endodontic treatment is to prevent the development of periapical lesions, as well as to create an environment conducive to their healing. To achieve such goals, it is necessary to adhere to certain classical principles of chemical disinfection and mechanical treatment of the root space. It is important to note that it is the success of the mechanical treatment of the endodontist that determines the effectiveness of all subsequent iatrogenic manipulations performed in the root canal.
For reliable obturation of the canal space with gutta-percha, it is necessary that it meet certain criteria, including:
- continuous conical shape of the main root canal, resembling a tapering funnel from the mouth to the apical foramen;
- narrowing of the cross-sectional diameter of the main canals in the apex area;
- preservation of the original shape of the channel during its processing;
- maintaining the original position of the apical foramen;
- maintaining the size of the apical foramen whenever possible.
The biological purpose of mechanical treatment of the endodontic space is as follows:
- restriction of the work of endodontic instruments within the boundaries of the root canal;
- prevention of extrusion of necrotic tissue into the postapical region;
- removal of all organic tissues from the space of the main and additional canals;
- creating a space of sufficient size to ensure effective irrigation and medicinal treatment without compromising the functional state of the tooth through excessive reduction in the thickness of dentin tissue.
Achieving the above goals in straight root canals is a fairly clear and logical process, however, in cases where there are various forms of anatomical variations in the endospace, this task becomes noticeably more complicated. It is especially difficult to achieve an adequate result of mechanical treatment of the canal in those with a pronounced bend of the endospace or in the presence of furcations and additional anastomoses (photo 1). It is quite difficult to follow classical intervention algorithms in such cases, therefore, to solve such problems, special NiTi files were developed, the sequence of application of which using the TCA technique helps to optimize the results of machining.
Photo 1a-c. Complex anatomical structure of root canals.
Treatment of canals with bends
Based on canal curvature, Nagy et al classified root canals into the following four categories:
- Straight or I-shaped (28% of root canals);
- Apically curved or J-shaped (23% of root canals);
- Curved along the entire length or C-shaped (33% of root canals);
- Multiple curved or S-shaped canals (16% of root canals).
Schäfer et al found that 84% of the root canals they studied were curved, while 17.5% had a second curvature and were classified as S-shaped. Of all the root canals with curves analyzed, 75% had a curvature level of less than 27°, 10% had a curvature ranged from 27 to 35°, and 15% had a pronounced curvature of more than 35°.
Traditionally, the severity of root canal curvature is described using the Schneider angle parameter: root canals with a bend of up to 5° are classified as straight canals, with a bend of 10 to 20° as moderately curved, and canals with a curve of more than 25° as severely curved. curved. Decades later, Pruett et al reported that two curved root canals can have the same Wein angle but completely different curvature parameters. To evaluate the latter, the radius of curvature parameter was introduced, which is defined as the radius of a circle passing through the curvilinear part of the channel. When using rotary tools, the number of cycles until the tool fails is significantly reduced as the radius of curvature decreases and the angle of curvature increases. Further attempts to mathematically describe the curvature of the channel on the basis of available two-dimensional radiographs led to the introduction into the theory of such parameters as the length of the curvature and its location, determined by the height and distance of the curvature. Estrela et al described a method for determining the radius of curvature of the root canal using CBCT slice data, which the scientists analyzed in specially developed software. According to their approach, the following three categories of root canal curvature were identified: small (r=4 mm), intermediate (r=4-8 mm) and large (r=8 mm). The smaller the radius of curvature, the greater its steepness. All of these attempts to describe root canal curvature had one goal: to develop an approach to assess the risk of apical foramen transportation and unexpected instrument separation.
Transport of channels and separation of instruments
According to the Glossary of Endodontic Terms, canal transport is the removal of the root canal wall structure on the outer side of the curvature in the apical half of the canal due to the properties of the files to restore their original linear shape. For stainless steel hand files and hand and machine NiTi files, the shape recovery properties are directly related to the size and taper of the tool. The larger the size and taper of the file, the more the file tries to restore its original shape, which is associated with an increase in the mass of metal in the structure of the tool. If the files exactly repeated the morphology of the endospace, then problems with transporting the canals would not arise at all, since in such an ideal situation the file would move strictly along the trajectory of the canal. Because the shape of the channels and instruments is different, each instrument moves along its own path within the curved channel, which is determined by its ability to recover. When attempting to increase the size of the apical foramen during mechanical treatment, as a rule, the amount of reduction of dentin tissue on the outer apical part of the curvature increases. To prevent this effect, doctors try to use instruments of a larger cone, but of a smaller size, for mechanical processing of the apical space in canals with pronounced curvature. Increasing the cone with this approach leads to a reduction in the angle of the bend, a decrease in its length and an increase in the radius with a reposition of the bend more apically (photo 2).
Photo 2. Treatment of the endospace leads to changes in bending parameters.
Reducing the volume of treatment of the apical part of the canal in those with pronounced curvature is indicated with the need to achieve the following goals:
- a smaller preparation diameter is associated with a smaller volume of canal wall reduction, a smaller increase in file size, and therefore with a lower risk of developing undesirable effects;
- files of smaller diameter are characterized by greater elasticity and less resistance to fatigue, thus, when working with these files, the possibility of transporting the canal as the size of the apical foramen increases is reduced.
The above-mentioned approaches to instrumental treatment of root canals, although safer, are also characterized by a number of disadvantages. Firstly, an increase in the taper of the endospace in its coronal part to ensure easier patency in the apical third provokes excessive reduction of dentin tissue, which compromises the biomechanical prognosis of the tooth. In addition, processing canals with smaller files makes it difficult for irrigation solutions to penetrate to the appropriate depth of the endospace. In canals with pronounced bends, the possibility of adequate irrigation of the root canal directly depends on the possibility of sufficient instrumental expansion of the apical third. Apical preparation of the apical part of the canal in order to achieve the appropriate level of disinfection in conditions of pronounced curvature is one of the most difficult practical tasks in endodontics, especially considering the prevalence of modern principles of minimally invasive interventions. In addition, there is a high risk of separation of rotary mechanical files in canals with pronounced curvature. The causes of such complications can be two main mechanisms: cyclic fatigue and torsion fatigue. When a rotary tool is activated within a curved channel, constant tensile and compressive stresses are generated within the physical center of rotation of the curvature. If the tip of the file is blocked in the endospace structure and the motor continues to rotate, the shear moment of the tool material exceeds its limit values, which also leads to the development of maximum levels of torsional fatigue (torsional fatigue). The greater the complexity of the morphology of channel bends, the fewer cycles of operation under such conditions the instrument can withstand.
Using Shape Memory Controlled Files
NiTi alloys are softer than stainless steel, but have a lower level of elasticity (about one-fourth to one-fifth that of stainless steel). At the same time, this material is more durable, rigid and elastic, due to which NiTi files are characterized by shape memory. NiTi files used in endodontics contain approximately 56% nickel and 44% titanium. However, they can exist in the form of two different temperature-dependent crystal structures called martensite (low-temperature phase) and austenite (high-temperature phase). The lattice organization can be transformed from austenitic to martensitic state by controlling temperature and stress. During the reverse transformation, the alloy passes through an unstable intermediate crystallographic phase called the R phase. The use of files during endodontic treatment provokes the development of stress, which, in turn, causes an instantaneous martensitic transformation of the NiTi file. A change in the shape of a tool is associated with a change in the parameters of its volume density. It is this property of the file, which is the ability to withstand stress without developing permanent deformation, that is called superelasticity. Superelasticity is most pronounced at the beginning of stress development, when the tool can easily overcome up to 8% deformation. After 100 deformations, this level drops to 6%, and after 100,000 – to 4%. It is within these boundaries that the shape memory effect is observed. In addition to stress, martensitic transformation of a file can also be caused by temperature changes. When the austenitic phase of a NiTi file cools, it begins to transform into martensitic phase. The temperature at which the martensite phase is completely restored again is called the temperature of the final transformation of martensite. When the martensite phase is heated, it begins to transform into the austenite phase. The temperature at which this phenomenon begins is called the temperature at which the austenite phase begins. At the final transformation temperature of austenite and above (Af), the material completes its shape memory transformation and demonstrates its superelastic properties. Until 2011, the Af temperature for most available NiTi tools was at or below room temperature. As a result, during clinical use, conventional NiTi files were in the austenitic phase, exhibiting their shape memory and superelasticity properties. In 2011, COLTENE introduced controlled shape memory files (CSF). The production of these tools involves the implementation of a unique thermomechanical process that controls the memory of the material, providing special elasticity and durability of the files, which is not typical for all other types of NiTi analogues. The Af-transformation temperature of CPF files is clearly higher than body temperature, as a result of which these files are in the martensite stage during operation in the endospace. In this phase, the instruments remain soft, plastic, without shape memory, and can be easily deformed, but after that they restore their shape and original elastic properties when heated to temperature Af.
A hybrid martensitic microstructure, like that used in HyFlex CM (COLTENE) files, also has a higher level of strength than an austenitic microstructure. At the same stress intensity, the rate of crack propagation in the structure of the austenitic phase is much higher than in the martensitic phase. A quantitative model for studying the process of crack development in the file structure made it possible to establish that the martensitic transformation of NiTi files increases the fracture strength of the tool by 47%.
More recently, the thermomechanical processing mechanism of CM has been combined with the mechanical fabrication procedure of NiTi files. Thanks to electrical discharge machining (EDM), it was possible to increase the surface hardness of files, their cutting efficiency and achieve unique parameters of resistance to functional fatigue. In the first published paper that demonstrated the results of using these files, the surface of the instruments was described as typical after an intrinsically safe specific treatment, and the level of degradation remained quite low even after multiple endodontic procedures. The authors also found that these files have surprisingly high levels of resistance to cyclic fatigue, and have a high safety profile even when working in highly curved canals, which has been confirmed in laboratory conditions. Pedulla et al also reported higher fatigue resistance values for HyFlex EDM (COLTENE) files, even compared to reciprocating machining and M-wire files.
Unfortunately, the literature data concerning the study of flexural stiffness and fracture resistance during the development of cyclic fatigue were carried out on NiTi files at room temperature. However, room temperature is not clinically significant. The use of modern instruments takes place at body temperature, which automatically excludes the possibility of direct application of the findings of previous studies in clinical practice. It is apparent that the transformation temperature (Af) of NiTi files designed for rotary or reciprocating processing can influence their clinical behavior under normal human body temperature conditions. Hulsmann et al (2019) reported that ambient temperature has a 500% influence on the service life of endodontic instruments. If the transformation temperature approaches body temperature, this can cause tools to appear flexible and fatigue resistant, but in fact become more rigid and less fatigue resistant. The Af of HyFlex EDM files was found to be close to 52°C, which is much higher than body temperature. Temperature analysis of EDM files confirmed the presence of a monoclinic structure of B19 martensite and a rhombohedral R phase. Thus, EDM instruments are always in the rhombohedral R-phase and martensitic crystallographic state at clinically relevant temperatures during endodontic treatment. The martensitic structure at body temperature allows these files to have excellent flexibility and resistance to fracture, as well as the absence of restoring forces, making them ideal for use during the machining of curved or morphologically complex canals.
Sequence of using HyFlex EDM Max files when processing curved canals
EDM technology has made it possible to implement the principle of endodontic expansion with a single rotary file. Generally, in most clinical cases, a 25/~ HyFlex EDM OneFile can be used with short peck movements while being sure to keep the instrument edges clear of debris and provide adequate irrigation. The OneFile is characterized by a size of 25 with a taper of 0.08. In this case, the taper of 0.08 is constant in the upper apical 4 mm of the instrument, but gradually decreases to 0.04 in the coronal part of the instrument. The file is characterized by the presence of three different cross-sectional zones along the entire length of the working part (rectangular in the apical part and two different trapezoidal cross-sections in the middle and coronal parts of the instrument). Thus, the developers managed to increase the file’s resistance to destruction and its cutting efficiency. When wider apical preparation is required, the designer introduces the following three HyFlex EDM finishing files with constant taper (40/.04, 50/.03 and 60/.02). For narrowed and obliterated canals, as well as for thin, long and S-shaped canals and canals with more than a 27° bend and a radius of curvature of less than 5 mm, a single file protocol is not indicated. In such cases, it is necessary to combine tools in order to achieve the most predictable treatment result. This is why the developer has also provided the Max Curve HyFlex EDM tool sequence, which includes files 15/.03, 10/.05 and 20/.05. The use of these files allows us to minimize the process of increasing the taper of the endospace, thus ensuring the minimum possible reduction of dentin on the canal walls. The Max Curve HyFlex EDM tool sequence can be used with the tactile controlled activation technique. Once the canal is identified, the minimal carpet is recreated using a 10/.02 stainless steel hand file. The 15/.03 HyFlex EDM tool is then used to follow the path of the carpet. After this, the 10/.05 HyFlex EDM file is used to widen the middle part of the canal. The apical 3 mm of the 10/.05 file act as a guide tip (without adhesion to the canal walls, photo 3). File 20/.05 HyFlex EDM is used as a final file to achieve the final smooth shape of the canal. After expansion with a 20/.05 instrument, the canal can be obturated with a 20/.05 gutta-percha cone and GuttaFlow biothermal sealer (COLTENE). The file sequence is easy to remember and ensures efficient and safe treatment of the endospace even in the most difficult clinical situations.
Photo 3. Sequence of HyFlex EDM Max Curve files.
Tactile control activation
In order to minimize the approach of using files with increasing taper, a tactile-controlled activation technique was proposed (photo 4a). This mechanical endospace technique can be defined as activating the stationary file only after it has been completely inserted into the patent canal. Essentially, the activation of the file occurs after the tactile sensation of achieving maximum adhesion of the cutting grooves to the walls of the endospace. Passive (non-activated) application of files is also useful, especially in cases of limited oral opening and incomplete visualization of the working field. Tactile-controlled activation can be classified into that during tool movement and during tool withdrawal. After creating access to the pulp cavity and localizing the mouths of the canals, their patency is ensured by the 10/.02 instrument. After this, the 15/.03 file is installed in the tip and inserted into the endospace until maximum resistance is felt (point A, photo 4b).
The file is then activated and pushed in the apical direction until the activated file reaches the point of resistance (point B, Fig. 4c). After this, the file is removed from the channel. The cutting edges of the instrument are cleared of debris, checked for deformations, and irrigation of the endospace is provided. The second time the same file is introduced, which can now go deeper in a passive state (point B, photo 4d). Re-activating the file will allow the file to advance the required length closer to the apical foramen (point C, photo 4e–g). Work with this tool is stopped only after it reaches the working length (point D, photo 4h). After reaching the working length, begin using the second file in the Max Curve sequence according to the protocol described above.
Photo 4a-h. Tactile controlled activation.
The thin apical 2 mm of a 10/.05 file will always remain free within the canal, which guides the file along the path of the endospace anatomy without the risk of developing excessive retention and breakage. File 20/.05 will ensure the final formation of the endospace and the conditions to ensure its proper disinfection and obturation. Mechanical processing of wider apical openings is achieved by increasing the width of the instruments used in particularly complex canals, such as those shown in photos 5 and 6; The use of a 20/.05 file would be most indicated, given the need to achieve proper disinfection of the endospace and minimize the risk of instrument separation. The TKA technique aims to minimize the time it takes to expand the endospace with an activated file, using file activation only when necessary to advance the instrument. With this approach and through the use of HyFlex EDM Max Curve files in a sequential manner, most anatomical variations of root canals can be treated without compromising the safety profile of the procedure.
Photo 5a-g. Treatment of the S-shaped mesiobuccal canal of the maxillary second molar using HyFlex EDM Max Curve files using the TKA technique: a) pre-treatment radiograph; b) radiograph after treatment; c) formation of the access cavity; d) view after processing with HyFlex EDM 15/.03 file; f) processing with HyFlex EDM 20/.05 file; f) obturation with gutta-percha pins 20/.05; g) view after obturation.
Photo 6a-d. Treatment of the S-shaped mesial canal of the mandibular second molar using HyFlex EDM Max Curve files: a) visualization of deep carious lesions; b) view after processing with HyFlex EDM 15/.03 file; c) view after obturation; d) view after restoration.
conclusions
NiTi files with CM effect are extremely flexible and have excellent fatigue resistance. They can be activated within the canal and passively moved along the bending path, guided by the original anatomy of the endospace. The TKA technique allows minimizing the time of close interaction of files with root dentin. During mechanical processing of the endospace, constant feedback tactile control of the manipulation is provided. For particularly complex clinical cases, a special sequence of HyFlex EDM Max Curve files has been developed, allowing clinicians to stay in tune with constantly moving progress.
Author: Dr Antonis Chaniotis (Greece)
Tooling methods
There are two methods of mechanical treatment of tooth canals:
- Apical-coronal – Step back. It consists of passing the root hole to the apex (physiological narrowing) with small reamer and subsequent expansion of the canal. The procedure is carried out in several stages, each of which uses larger files.
- Coronary-apical – Crown down . To pass through, the largest possible file is used first, and for further cleaning, tools are used in descending order of their size.
Important! At the end of the procedure, the canal should acquire a cone-shaped shape and its size should increase.
Stages of pulpitis treatment.
The first method is usually used when the roots are too thin, and their excessive expansion can lead to perforation (the formation of a pathological hole in the tooth cavity). Regardless of the method, at each stage of cleaning and expansion, antiseptic treatment of the root holes is carried out.
Today, advanced dentistry uses treatment under a microscope. It allows you to visually monitor each stage of therapy, adjust the position of the instruments and significantly reduce the likelihood of error.
Recommendations after treatment
Endodontic treatment demonstrates high success rates. After the intervention, you must adhere to the following recommendations:
- Avoid too hot, spicy, or cold foods for several days (while teeth sensitivity remains).
- Maintain good hygiene – brush your teeth twice a day, use dental floss and an irrigator.
- Do not chew anything hard (do not chew nuts, candies, etc.), as this may result in damage to the root canals and tooth destruction.
- Undergo medical examinations with a dentist and hygienist (at least 2 times a year).
Immediately after the procedure, tooth sensitivity increases greatly. This is explained by the reaction of the tissues to the filling material. The discomfort will disappear in a few days.
Types of filling materials
When filling a canal, one of the following types of materials can be used:
- Plastic non-hardening. They consist of an active component (calcium hydroxide, antiseptic, antibiotic or corticosteroid) and a filler (white clay, aromatic oil, zinc oxide). They are used for temporary filling.
- Plastic hardening. They are pastes based on zinc oxide eugenol, calcium hydroxide, resorcinol-formalin, epoxy resins or glass ionomer cement.
- Solid or pins. Divided into two groups:
- plastic: plastic, gutta-percha, fiber;
- non-plastic: metal, plastic, fiberglass, Thermafil system (a metal rod on which gutta-percha is applied).
Regardless of the method, at each stage of cleaning and expansion, antiseptic treatment of the root holes is carried out.
Important! The most popular and high-quality filling methods are using gutta-percha and the Termafil system.
High demands are placed on filling materials. They have to:
- easy to insert and, if necessary, remove from the canal;
- appear on X-ray images;
- do not cause allergies or tissue irritation;
- do not dissolve, do not shrink, do not change volume and do not stain dental tissues;
- fits well to the walls of the roots;
- have an antibacterial and antiseptic effect.
Removal of filling material beyond the apical foramen during obturation of the Root Canal
Penetration of the filling material (sealer) beyond the apical hole is often considered acceptable, and the surrounding tissues are quickly restored if a high-quality disinfection of the root canal has previously been carried out. Some American colleagues even suggest that filling the root canal beyond the apical foramen, which is noted on the control radiograph in the form of a small “nodule” (“Puff”), is a sign of a very high-quality sealed root canal. It is possible that if mechanical treatment was previously carried out to create apical patency (“Patency”) and subsequent thorough disinfection of the root canal, then the marginal fit of such a root filling will be better in the apical region due to the lower likelihood of apical microleakage (“Leakage”)... But this has not yet been proven. On the other hand, studies have shown (Peng et al., 2007) that when filling material was moved beyond the apical foramen, treatment success rates decreased by 28%.
From all of the above, it follows that in endodontics there is very little data confirmed by evidence-based medicine.
Summarizing the topic, Prof. Hülsman noted that a slight release of the sealer beyond the apical hole when filling the root canal does not cause harm. However, pushing dentine filings beyond the apical hole, as well as slightly pushing the root filling beyond the apical hole can lead to pain, which, fortunately, usually disappears on its own. Deliberately carried out mechanical development of the root canal beyond the apical foramen using instruments of sizes 08, 10 and 15 according to ISO leads to such minor trauma to the apical periodontal tissues that long-term pain for this reason alone should generally not arise.
But prof. Hülsman cautioned that the disadvantage of using the modern Patency method is still the risk of pushing infected dentin beyond the apical foramen. The speaker went on to quote from a fairly old study (Torneck et al., 1973): “Occlusion of the apical part of the root canal with infected dentin filings impedes tissue healing in the apical region.”
Thus, regarding the use of the technique of creating apical patency (“Patency”), a final point of view has not yet emerged.
Cost of root canal treatment in Moscow
The price of endodontic treatment depends on the number of root canals of the diseased tooth, the method used, complexity (including re-treatment) and volume of intervention, type of filling, etc. Processing 1 channel requires less work than 2 or 3, which affects the cost.
| Group of teeth | Cost of pulpitis treatment | Cost of periodontitis treatment |
| 1 canal tooth | 6500 rub. | 8500 rub. |
| 2 channel tooth | 7500 rub. | 9500 rub. |
| 3-channel tooth or more | from 8500 rub. | from 10,500 to 12,000 rub. |
The price includes the entire list of procedures performed for the treatment of dental canals. When using a dental microscope and laser equipment in complex therapy, the cost of treatment increases.
Stages
There are several ways to treat root canals. One method or another is selected based on the clinical picture and technical capabilities of the clinic. However, each of them includes several key steps:
- Diagnostics. Radiography is usually used to determine the area of the lesion and confirm the diagnosis. Sometimes electroodontodiagnosis is used to identify the sensitivity of the pulp.
- Anesthesia.
- Isolation of the tooth with a rubber dam - a latex handkerchief.
- Cleaning the coronal part of the tooth from carious lesions and providing access to the pulp chamber. You may have to remove some healthy tissue to get to the root holes.
- Pulp extirpation. It is carried out mechanically using special tools (files, reamers) with simultaneous antiseptic treatment.
- Cleaning and expansion. For this purpose, files, reamers or an acoustic endodontic system equipped with abrasive instruments are used. This stage should take place under radiographic control. It is necessary to determine the length of the root holes, their structure, as well as to determine the depth of penetration.
- Filling. The channels are filled with special hermetic connections or pins.
- Restoration of the crown part of the tooth.
There are several ways to treat root canals.
Important! It is not necessary to use a rubber dam when removing caries-affected tissue. But it is necessary during cleaning and filling to prevent bodily fluids and dirt from entering the cavity.
Root canal treatment is carried out over 3 visits. In the first, the pulp and affected tissues are removed, in the second, the root holes are filled, and only then the crown is restored.