Why is anatomical knowledge needed in cosmetology?
Modern cosmetic procedures cannot be carried out without basic knowledge of the anatomy and physiology of the skin.
This information allows the cosmetologist to correctly work on age-related changes in the skin, qualitatively improve its general condition and carry out timely work with the facial muscles, influencing them with the help of massage movements when performing cosmetic manipulations.
The structure of facial skin muscles, studying their descriptions from photographs and diagrams is basic knowledge of anatomy. Without them, not a single cosmetologist will be able to competently perform a massage, inject Botox under the skin of the face without negative consequences, or perform a microcurrent therapy procedure.
Anatomical and physiological features of the maxillofacial region
ANATOMICAL AND PHYSIOLOGICAL FEATURES OF THE MAXILLOFACIAL AREA
The area of the face and oral cavity consists of organs and tissues, the anatomical, topographical and functional features of which are characterized by close interconnection and even interdependence. In terms of length and volume, a large proportion of the anatomical region falls on the masticatory apparatus, which is the initial section of the digestive system. The rest of the maxillofacial region is represented by the sensory organs, speech, and upper respiratory tract.
The presence within a relatively small anatomical zone of organs that are so important and at the same time so diverse in their functions constitutes its essential feature. The structure of the facial skeleton and ligamentous apparatus is also characterized by a complex relationship. The topographic-anatomical and functional diversity of muscles, integumentary tissues, the abundant innervation, blood supply and lymphatic drainage pathways of organs and tissues - all this makes it possible to distinguish the maxillofacial region as one of the most complex and requires deep knowledge from a clinical doctor.
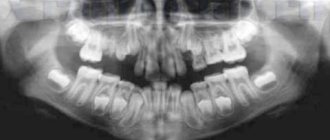
The bony skeleton of the face consists of 6 paired and 2 unpaired bones: 2 maxillary (os maxilla), 2 shark (os zigomaticus), 2 palatine (os palatinum), 2 nasal (os nasalis), 2 lacrimal (os lacrimale), 2 nasal turbinates (concha nasalis), 1 vomer (vomer) and lower jaw (os maxilla). The bones that form the facial skeleton are immovably connected by bone sutures to each other and to the base of the skull. The lower jaw is the only movable bone of the facial skeleton. It is connected to the base of the skull by a complex temporomandibular joint. The lower jaw, due to the peculiarities of the temporomandibular joint, moves in three planes and consists of a body with an alveolar process and two branches extending from the body at different angles and ending with the condylar and coronoid processes. The body of the jaw is formed by 2 plates (external and internal) of compact bone substance, the space between which is filled with spongy bone. The mandibular canal runs throughout the body of the jaw, having different positions in relation to the lower edge of the jaw and the roots of the teeth. Inside the alveolar process are the roots of falling out (baby) or permanent teeth, the crowns of which stand freely in the oral cavity. The grooved depression located between the tooth and the free edge of the gum is called a gum pocket.
A tooth (dens) consists of a dental crown (corona dentis), a neck (collum dentis) and a root (radix dentis). The root ends at the apex (apex radicis), on which there is a small hole - foramen apicis. Through this hole, blood vessels and nerves enter the tooth.
The muscles of the maxillofacial region are divided into facial and chewing muscles.
The facial muscles are located relatively superficially under the skin. Their function is related to the physical and mental state of a person. Some of them are involved in the expansion or narrowing of the natural crevices of the face: mouth, nose, eyes.
The group of masticatory muscles includes the masticatory muscle itself (m. masseter), the temporal muscle (m. temporalis), and the external and internal pterygoid muscles (mm. pterygoideus medialis et lateralis). This group of muscles lifts the lower jaw up, pushes it forward and to the side. Three muscles of the suprahyoid region—the anterior belly of the digastric muscle (venter anterior m. digastricus), the geniohyoid (m. geniohyoideus) and the mylohyoid (m. mylohyoideus)—carry out the downward movement of the lower jaw.
The group of muscles that lift the mandible is conventionally classified as the posterior group, and the releasing muscles are classified as the anterior group of the masticatory muscles, or muscles of the lower jaw.
The integument of the maxillofacial region, both skin and mucous membranes, is characterized by great mobility. This mobility is due to their elasticity, as well as the presence of a well-defined layer of loose subcutaneous and submucosal fatty tissue. The mucous membrane is not equally mobile everywhere. In the area of the alveolar processes and hard palate, it is completely devoid of submucosal fatty tissue, and, therefore, in these anatomical areas there is no mobility of the mucous membranes. The mucous membrane of the oral cavity and oropharynx is covered with stratified squamous epithelium, which (unlike the epithelium of the skin) lacks hair follicles, sweat glands and the stratum pellucida. The thickness of this epithelium is usually greater than that of the skin. Only in areas that are actively involved in the act of chewing does the epithelium undergo keratinization. Mucous and serous glands are located mainly under the non-keratinizing epithelium. The proper layer of the mucous membrane consists of loose connective tissue, located superficially between the epithelial outgrowths and in the deeper parts passing into the fibrous-fatty tissue of the submucosa.
Organization of the work of the department of surgical dentistry
The color of the red border of the lips is due to the presence of long epithelial processes, between which are located high, richly vascularized connective tissue papillae of the own layer of the mucous membrane.
The buccal submucosa contains a significant amount of adipose tissue; the layer of the mucous membrane itself has a loose consistency. The epithelium is non-keratinizing.
The gingival epithelium on the vestibular side has more pronounced signs of keratinization than on the lingual side. In the presence of teeth, the stratified squamous epithelium turns into a rudimentary odontogenic epithelium, which is attached to the circular ligament; After teeth fall out, this feature disappears.
In the anterior part of the hard palate, keratinization is more pronounced; individual epithelial pearls are located along the midline, indicating the site of embryonic fusion. The submucosa of the hard palate is dense, contains a lot of collagen and minor salivary glands, especially at the border with the soft palate.
The dorsum of the tongue is covered with a thick epithelium, and there are special papillary elevations and taste buds on it. The ventral surface is smooth and similar to the mucous membrane of the floor of the mouth and cheeks.
The oral cavity (cavum oris) is divided into two sections: the vestibule of the mouth (vestibulum oris) and the oral cavity itself (cavum pros proprium). The vestibule of the mouth is located between the lips and cheeks on the outside, and the teeth and gums on the inside. Through the oral opening (rama oris), the vestibule of the mouth opens outward.
The tongue (lingua) is a muscular organ. There is a body of the tongue (corpus lingua), a tip (apex) and a posterior part - the root of the tongue (radix lingua). The excretory ducts of three pairs of large salivary glands open into the oral cavity: parotid (glandula parotis), submandibular (glandula submandibularis) and sublingual (glandula sublingualis).
Blood supply. The rich vascularization of the maxillofacial region plays an important role in increasing the regenerative capacity of tissues. Abundant blood supply comes from the external carotid artery, which provides a dense network of vessels that communicate with each other. Some of them, with a fairly large lumen, pass directly under the skin: the facial artery (a. facialis), the superficial temporal artery (a. temporalis superficial) and the facial vein (v. facialis). It should be noted that individual anatomical organs of the maxillofacial region, in particular the lower jaw, have several sources of blood supply.
The venous system of the face is built like an arterial one. Its main branches are the facial and retromandibular veins (vv. facialis et retromandibularis), which collect blood from smaller veins. The pterygoid venous plexus (plexus venosus pterygoideus) is located in the infratemporal fossa. The venous vessels of the face widely anastomose with each other and have connections with the cranial cavity and the cavernous sinus (sinus cavernosus).
The lymphatic system of the facial area is well developed, ensuring the outflow of lymph from the tissues and organs of the oral cavity and face. Lymph on its way passes through the lymphatic facial, submandibular and cervical nodes, through the lower deep cervical nodes and enters the truncus jugularis.
Innervation of the maxillofacial region. It is carried out mainly by the trigeminal (n. trigeminus), sublingual (n. hypo-glossus), facial (n. facialis), glossopharyngeal (n. glossopharyngeus) nerves and nerves arising from the cervical plexus.
Organization of the work of a surgical dental hospital
Functions of the oral cavity. The oral cavity and its surrounding organs are of great importance in the implementation of the most important life functions. It is involved in digestion, respiration, voice and speech formation. The salivary glands are not only exocrine glands, but also excretory and internal secretion organs. The mucous membrane contains various sensory organs - receptors.
When food enters the oral cavity, complex motor acts occur: chewing, sucking and a secretory act - salivation. Food, while in the human oral cavity, is subjected to mechanical and chemical processing, after which the third act occurs—swallowing.
Chewing is a reflex motor component of the act of eating. During chewing, a person undergoes many different movements of the lower jaw. These movements are ensured by the special structure of the temporomandibular joint, the location and direction of traction of individual groups of masticatory muscles. Taking into account the movements of the lower jaw plays an important role in the general assessment of the act of eating and the function of the masticatory apparatus.
Sucking in an adult is important mainly when taking liquids. Hermetic closure of the oral cavity occurs due to the fact that the tip of the tongue is raised on both sides, pressing against the back teeth and the corresponding parts of the upper jaw, the lower surface of the tongue lies on the edge of the lower jaw, and the soft palate is extended downwards over the root of the tongue.
After chewing and mixing with saliva, the bolus of food passes into the stomach. This occurs as a result of a complex motor act - swallowing.
Swallowing is a bilateral, coordinated act, which involves a large number of muscles that contract strictly in concert and in a certain sequence. The mechanism of swallowing consists of peristaltic muscle movement, through which the bolus of food gradually moves forward, entering the esophagus and gastrointestinal tract.
From the oral cavity, as the initial part of the digestive tract, reflex effects are exerted on the secretion of the salivary glands and glands located in the abdominal cavity, on the motor work of the smooth muscles of the stomach and intestines. With the participation of the oral and nasal cavities, gas exchange occurs between the body and the external environment. Through the oral cavity, substances necessary for the preservation and development of life enter the body. The organs of the oral cavity take part in the formation of voice and articulate speech.
Which facial muscles are injected with Botox?
The introduction of Botox is aimed at eliminating facial wrinkles and restoring smoothness to the skin texture. Injections of botulinum toxin (purified natural protein) are performed by a cosmetologist subcutaneously or intradermally into the facial muscles.
These are the muscles where it is necessary to reduce susceptibility to incoming nerve impulses in order to slow down the process of deepening wrinkles in the skin and tighten sagging skin.
Botulinum toxin injections best show their effect in the following muscles:
- in platism;
- in the muscle that depresses the corners of the mouth;
- in the orbicularis muscles of the mouth and eyes;
- in the mental muscle;
- in the nasal muscle;
- in the frontal muscle;
- in the pride muscle and the corrugator muscle.
The amount of the drug for each muscle zone is determined individually by the cosmetologist performing the procedure for introducing Botox under the skin. The maximum effect of “freezing” of facial muscles is observed for 3-6 months after the injection.
As soon as the muscles begin to make the first contractions, after this period of time, the effect of botulinum toxin injections under the skin lasts for about six months.
The facial muscles (photos with descriptions and diagrams can be seen above) should be studied using the photographs and diagrams presented. The diagrams are presented in Russian and Latin. On them you can see a detailed description of where this or that group of facial muscles is located.
If you know the exact location of the facial and neck muscles and familiarize yourself with the principle of their work, understanding this by studying descriptions, photographs and diagrams, then you can, through subsequent competent stimulation of certain muscle groups, slow down the aging process, maintaining the elasticity and youth of the skin for a long time.
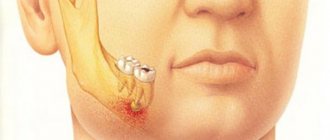
Fracture - what are the symptoms of damage?
It is rare to see a fracture or damage to the hyoid bone, but you need to understand that this can happen if you receive a trauma to the lower jaw. To cause injury to this area, a strong mechanical impact must be exerted on it. There are cases when such a fracture becomes the cause of strangulation, as, for example, occurs during hanging.
You will learn about such a fracture immediately, since the symptoms are considered quite vivid:
- Severe pain will occur in the front of the neck when swallowing and chewing food.
- A small hematoma will be visible in the area of the hyoid bone.
- When palpated, you will feel the mobility of the debris.
When the injury to a given bone is more severe, the mucous membrane ruptures. Therefore, quite severe bleeding from the mouth occurs if the branches of the lingual or thyroid artery are affected. In most cases, such an injury leads to death if the moment is missed before emergency assistance is provided.
However, first aid measures may not always be successful. Experts confirm the fact that all injuries that are associated with damage to the hyoid bone and mylohyoid muscle are more than dangerous to human health and life.