What types of tooth-saving operations are used in dental practice?
- Hemisection is an operation to remove part of a tooth and its root, the treatment of which is not possible. The remaining part of the tooth is used for further procedures to restore the dentition.
- Flap tooth-preserving operations - this type of surgical intervention is effective for periodontal diseases. Manipulations help prevent further destruction of bone tissue and the ligament that holds the teeth.
- Root apex resection is a type of tooth-saving operation when the upper part of the affected root is cut off, tissue decay products are removed, and the resulting cavity is filled with bone material. With this intervention, the tooth completely retains its strength and can be used for further prosthetics.
- Cystectomy is a procedure that allows you to completely remove a cyst or granuloma. Typically, along with this surgical intervention, resection of the root apex is performed, after which the resulting empty space is filled with artificial bone tissue. Before performing a cystectomy, the canals of the tooth that is causing the cyst are re-treated and filled; this type of treatment, as a rule, only applies to single-rooted teeth.
- Cystotomy is a cyst treatment method that involves partial removal of the cyst, which removes the anterior wall of the cyst and creates a connection with the oral cavity. This method is used when the size of the cyst is such that it involves several teeth, which may not even have been previously treated. The preparatory procedure is the same as during a cystectomy, re-treatment and filling of the causative tooth; the remaining teeth are not affected. After manipulation, the tumor is significantly reduced in size.
TOOTH-PRESERVING OPERATIONS
Resection of the root apex.
Endodontic preparation of the tooth for surgery (mechanical, medicinal treatment of the tooth canal, filling the canal with Thermafil). An arcuate or trapezoidal incision of the mucous membrane and periosteum with the formation of a mucoperiosteal flap within three teeth with the base to the transitional fold. The soft tissue is separated from the bone using a raspatory
along the entire length of the wound and pull them to the base of the flap with a flat or blunt serrated hook. All manipulations on bone tissue and roots are carried out with a spherical or fissure bur. With the help of burs, the existing usura is expanded until the apical part of the root is exposed within the boundaries of the defect existing in the bone. The modified root tip is separated with a fissure bur down to its sealed part. If the root canal at the resection site is without filling material, retrograde filling is performed. Using a curettage spoon, a smoothing spoon or a narrow rasp, the granuloma or pathological granulation tissue is removed along with the resected root tip. The walls of the defect in the bone are scraped out. The bone and soft tissue wound is irrigated with an antiseptic solution. The mucoperiosteal flap, detached and held with a hook, is placed in its original place. Interrupted sutures are placed on the edges of the soft tissue wound. A pressure bandage is applied to the facial skin corresponding to the area of surgery for 10-12 hours.
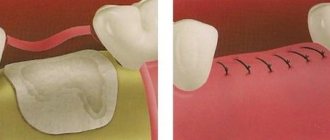
Tooth root amputation.
Tooth root amputation is understood as cutting off and removing the entire root at the point where it departs from the bifurcation (trifurcation) without violating the integrity of the coronal part of the tooth. The operation is performed on the molars of the upper jaw in various ways: removal of one or both buccal roots or one palatal root. Less commonly, this operation is performed on the premolars of the upper jaw, when one of the roots is removed. An incision is made and the mucoperiosteal flap is peeled off so as to create more convenient access to the amputated root and bifurcation of the tooth root. Hemostasis is carried out. A thin fissure bur is used to remove part of the alveolus in the area of the amputated tooth. The root of the tooth is sawed off and removed with forceps or an elevator. Curettage is performed in the area of the socket of the removed tooth root. Diamond burs, shaped heads, and cutters are used to level the overhanging edges of the tooth in the area of its neck and alveoli. Hemostasis and wound care are carried out, and if necessary, retrograde filling is performed at the site of tooth root removal with silver amalgam.
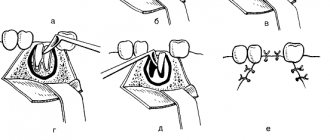
Hemisection of the tooth root.
Tooth root hemisection refers to the cutting off and removal of one of its roots from the tooth along with the adjacent part of the tooth crown. The operation is performed on the molars of the lower jaw, less often on the premolars of the upper jaw. The operation can be performed with or without peeling of the mucoperiosteal flap. The latter technique is more traumatic and is used
rarely. An incision is made and the mucoperiosteal flap is peeled off so as to provide a good overview of the surgical field, especially the area of the bifurcation of the tooth root. Using a diamond disk and thin fissure burs, the tooth crown is dissected through the bifurcation zone so as not to injure the interradicular septum and alveolar walls. Using forceps or an elevator, one of the roots of the tooth is removed along with the coronal part adjacent to it and the hole is curetted. Hemostasis is carried out. Using diamond shaped heads and burs, the overhanging edges of the coronal part of the tooth adjacent to the wound are smoothed. Final hemostasis and wound care are performed. The mucoperiosteal flap is placed in the correct position and secured with sutures. A sterile gauze ball is applied to the wound for 10-15 minutes.
Coronoradicular separation.
The operation is performed on the molars of the lower jaw. An incision is made and the mucoperiosteal flap is removed so as to provide a good view of the bifurcation site. Using diamond discs, burs and shaped heads, the tooth is sawed in half and the overhanging edges of the coronal part of the tooth are smoothed. Curettage is performed in the area of bifurcation of the tooth root. Hemostasis and wound care are performed. The mucoperiosteal flap is placed in its original position and fixed with sutures. A sterile gauze ball is applied to the wound for 10-15 minutes. Subsequently, crowns are made for each fragment of the tooth crown and soldered together.
Replantation of teeth.
The tooth to be replanted is carefully removed so as not to damage the tooth and its socket. The extracted tooth is immersed in an isotonic solution of sodium chloride with antibiotics. Pathologically altered tissues are removed from the socket, preserving the periosteum. Cover the hole with a sterile swab, which the patient holds with his jaws closed. The apex of its roots is resected, the root canals are expanded and processed from the apex side, and they are filled. The tooth is inserted into the hole, placed in the same position, and fixed. Additional fixation of the tooth with a splint or ligature is carried out in cases where the tooth does not fit tightly into the socket. To secure the replanted teeth, an individually made bent wire splint is used, which is reinforced with ligature wire. This splint provides reliable fixation of the replanted tooth and creates support for it. A quick-hardening resin can be used to secure the tooth.
plastic. Replanted multi-rooted teeth, in the presence of neighboring ones, are often firmly held without additional fastening. Complete healing of the transplanted tooth occurs in 4-6 weeks.
Contraindications to tooth-preserving operations:
- Fused dental roots that are difficult to separate.
- Significant changes in bone tissue in the area of the inflammatory process.
To perform tooth-preserving operations, Medikastom dentistry uses effective and modern surgical methods. To get advice on their use or make an appointment, please contact us by phone.
Our 24-hour dentistry provides the widest range of services. We are always ready to provide you with services such as the selection of individual hygiene products and professional oral hygiene.
Concept and essence
Tooth-preserving operations are called operations aimed at preserving even, at first glance, a hopeless element of the jaw row.
The alternative is removal and subsequent installation of an implant or bridge, which is a much more time-consuming and costly option.
Most often, such manipulations are resorted to in the following cases.
- Progressive inflammation in the periodontium with resorption of the alveolar process, destruction of the periodontium, infection of neighboring units.
Deep pockets, granulating or granulomatous periodontitis, gum recession, instability of individual elements of the jaw arch - in all these cases, operations can restore the functionality of the organ for a long time, eliminating the need for implantation and prosthetics. - Root perforation. It usually occurs when the canals are unsealed or sealed inaccurately.
- Damage to units that serve as supporting elements for bridges and crowns. Their removal is undesirable, since it entails the manufacture and installation of new orthopedic structures.
- Pathologies in the bifurcation zone (the junction of the roots) of multi-rooted elements of the jaw arch.
Tooth-preserving operations can be therapeutic (conservative), surgical or mixed. Most often they are microsurgical interventions.
How is tooth-saving surgery performed?
Dental-preserving surgery is gentle in nature and at the same time it refers to a surgical intervention. That is why tooth-preserving surgery is performed under anesthesia: local or general.
Tooth-preserving operations can be aimed at replacing bone defects with drugs based on calcium hydroxide, as well as at regenerating bone tissue. In tooth-preserving operations, bone replacement drugs are used.
Dentists at the Dental Implant Center use the latest bone grafting technologies in their work, which achieves full compatibility and rapid restoration of tooth tissue.
After tooth-saving surgery, a caring dentist will prescribe special post-operative oral care for his patient, which will ensure rapid tissue healing. Physiotherapy, mouth rinse, and medication may be prescribed as follow-up care and treatment.
Dental-preserving operations are absolutely painless for the patient, and the time for complete rehabilitation and recovery is reduced to a minimum. The recovery period after tooth-saving surgery usually depends on the patient’s immunity.
After tooth-saving surgery, the patient is under close and constant supervision of the dentist. The dentist monitors the process of bone tissue restoration using x-rays, which are performed 1, 3, 6, 12 months after tooth-preserving surgery.
The most popular tooth-preserving operations
The most popular tooth-preserving operation is the operation to remove a dental cyst, which is performed using a cystotomy or cystectomy. The main advantage of this tooth-preserving operation is that removal of the cyst does not entail the removal of a healthy tooth.
The next most popular is tooth-preserving surgery, during which the roots of the tooth are removed. In many cases, tooth damage begins at the root, followed by destruction of the entire tooth. Tooth-preserving surgery is based on the fact that if one affected root is removed, a tooth with only 3 roots will retain its functionality.
With timely access to the talented and highly qualified specialists of the Dental Implant dental center, it is possible to save a tooth and relieve a person from toothache, which sometimes makes the patient’s life unbearable.
The next type of tooth-preserving operation is tissue regeneration, during which it is possible to restore missing tooth tissue, grow new bone, and restore damaged areas of the oral cavity.
Currently, vestibulloplasty has become popular - a tooth-preserving operation in which facial wrinkles are transferred from one place to another. Vestibulloplasty helps in correcting pathologies in the structure of the oral cavity, periodontal treatment, and implantation.