Cellular part of the dental pulp
The cellular part consists of many cells, the most important of which are:
- Fibroblasts occupy the central part of the dental pulp. Their function is to synthesize collagen;
- Odontoblasts consist of a pear-shaped or oval body and two processes: peripheral and central. The bodies of these cells border the dentin, and the peripheral processes lie in the dentinal tubules, completely filling their lumen. When dentin is damaged, odontoblasts are activated and begin the synthesis of tertiary (reparative) dentin;
- Histiocytes are wandering cells that transform into macrophages when needed;
- Undifferentiated mesenchymal cells can transform into any of the above cells;
- During trauma or inflammatory processes, lymphocytes, leukocytes, plasma cells , etc. can also be found in the dental pulp;
Structural features and functions
Pulp is loose connective tissue that includes various elements. This:
- odontoblasts, stellate cells, fibroblasts;
- elastin and collagen fibers;
- nerve endings;
- blood vessels.
The fabric consists of 74% water, the remainder consists of inorganic elements and organic compounds: proteins, amino acids, lipids, polysaccharides.
The structure of the pulp differs slightly in different parts of the tooth. The root pulp is relatively dense and contains a large number of collagen fibers. In the crown area, the pulp is soft and loose, penetrated by a branched network of capillaries and nerve fibers. In the anterior incisors and canines, the transition from the coronal to the root pulp is smooth. In chewing teeth, there is a clear boundary between loose and dense tissue - the mouths of the dental canals.
The pulp provides the basic vital processes of the tooth and performs several functions:
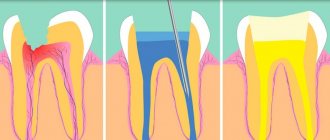
- plastic – stimulates dentin regeneration, the formation of replacement hard tissue in case of damage;
- protective – prevents infection from penetrating into periodontal tissues;
- sensory – transmits a signal about the influence of an external or internal irritant, thereby maintaining dental health;
- trophic – provides nutrition to dentin and tooth enamel.
Vessels of the dental pulp
The vessels of the pulp consist of arteries, arterioles, lymphatic vessels and veins that enter and exit the pulp chamber through the apical foramen.
Arteries and arterioles in the coronal part branch and form many capillaries. Capillaries are in close contact with odontoblasts, thereby providing the latter with nutrients.
Lymphatic vessels form blind sacs near the odontoblasts.
Waste products are removed from the dental pulp through veins through the apical foramen.
Innervation of dental pulp and dentin
Innervation of dental pulp and dentin . Bundles of pulpy nerve fibers enter the apical foramen of the root along with blood vessels, forming the already mentioned neurovascular bundle. On their way through the root pulp, they give off a number of lateral branches that participate in the innervation of the layer of odontoblasts and blood vessels of the root pulp. However, the most extensive branching of the nerve trunks, as well as blood vessels, occurs during their transition from the root pulp to the coronal pulp, and especially in this latter (Fig. 79).
The bundles of nerve fibers, continuing to branch, give off thinner branches and individual nerve fibers, which are directed to the peripheral parts of the coronal pulp and form a dense plexus here. This plexus, located near the subodontoblastic layer of the pulp, is called Rashkov's plexus. It contains a large number of nerve endings related to the innervation of both the pulp itself and the internal parts of the peripulpal dentin.
Despite the high pain and temperature sensitivity of the dental pulp, many authors denied the existence of special sensitive nerve endings in it. Only in the work of A. A. Manina the question was raised about the presence of receptor apparatus in the pulp, but a sufficiently clear description of their morphology was not given. Even more controversy and disagreement arises regarding the sensitive innervation of the dentin substance. While some authors believe that nerve fibers penetrate dentin almost to the border with the enamel and form sensitive nerve endings in it, others categorically deny the presence of nerve fibers in dentin. Finally, the third group of authors recognizes the existence of nerve fibers and endings only in the internal, non-calcified zone of dentin, the so-called predentin.
Our studies have shown that the dental pulp undoubtedly has its own receptors. Some of them are associated with the innervation of the layer of odontoblasts and dentin, and some are related to the innervation of connective tissue and blood vessels of the pulp itself. All of them belong to the category of branched bushes, with thin long branches running in different planes. Therefore, they are not always revealed in their entirety on sections. One of the bush-type receptors that we found in the pulp of the human incisor crown is shown in Fig. 80.
It is formed by a thick pulpy fiber which first divides into several large branches and then breaks up into a series of thin terminal branches which continue to branch in the peripheral parts of the coronal pulp. Some of the terminals of this receptor are directed to the odontoblast layer.
In some cases, the terminal branches of the pulp receptors terminate simultaneously in both the connective tissue and the pulp vessels. Endings appear that resemble polyvalent or vascular-tissue receptors of various internal organs (Fig. 81).
In addition, in the pulp there are special vascular receptors formed by nerve fibers, the terminal branches of which spirally entwine the walls of the blood vessels of the pulp. Of particular interest are the receptors that we discovered in the subodontoblastic layer of the pulp (Fig. 82 and 84).
They have the form of bushes, the terminal filaments of which pass through the layer of odontoblasts and penetrate into the predentine, where they can be traced to the border with the layer of calcified dentin. Many authors who observed thin nerve fibers in predentin and in the initial sections of dentinal tubules tended to consider them as independent nerve endings in dentin. In fact, many of them are only individual terminal filaments of cluster endings located in the subodontoblastic layer of the pulp.
Medical examination of children who have suffered trauma to the face and jaws
In addition to the endings mentioned above, the sensitive nature of which does not raise doubts, in the predentin and in the layer of odontoblasts there are also other forms of nerve endings, for which it is difficult to say whether they are sensitive or efferent (trophic) endings (Fig. 83 and 85).
The nerve ending shown in Fig. 83, is formed by a soft nerve fiber, which, having entered the predentin layer, turns to the side and runs parallel to the odontoblast layer, giving off thin lateral branches.
Some of them descend again into the odontoblast layer, and some end in the predentin substance. Similar endings were described in this layer of dentin by Calderon, Tiegs, A. A. Manina, I. M. Oksman, and more recently by Tserosi, Apwill, Vachek and Plachkova.
All the nerve formations described above were found by us in the pulp of the crown and partially in the neck of the tooth. As for the innervation of the root pulp, it has its own characteristics. First of all, there is no subodontoblastic nerve plexus of Rashkov, which is usually well developed in the pulp of the tooth crown. The bundles of nerve fibers running in the root pulp give off one after another a series of nerve fibers, which, arching and dichotomously branching, are directed to the odontoblast layer.
We, like other authors, were unable to detect any nerve endings in the predentin of the root canal wall. All this indicates a poorer innervation of the tooth root compared to the crown.
Thus, based on the data presented, we can conclude that the internal sections of the peripulpar dentin (predeitin) of the tooth crown have a well-defined sensitive and, possibly, efferent innervation. Evidence of this is the nerve endings, varied in structure, found by us and other authors in this layer of dentin. As for the possibility of penetration of nerve fibers into calcified dentin, it should be considered unproven. The data of a number of authors, who assumed massive penetration of nerve fibers into calcified dentin almost throughout its entire thickness, have been repeatedly criticized and can hardly be considered any convincing. Works of the last decade again speak of the possibility of penetration of individual nerve fibers into the tubules of calcified dentin or into its ground substance. All these works were performed using various methods of impregnation of nerves with silver. It is interesting to point out that none of the authors who were engaged in electron microscopic studies of the dentin of an adult developing tooth found nerve fibers either in the main substance of dentin or in its tubules.
Clinical examination of children with tumors in the maxillofacial area
In this regard, the question arises of how to explain the sensitivity of dentin and severe pain, which often arise when preparing a cavity in a tooth, if the nerve elements are absent in calcified dentin, but are present only in the inner zone of peripulpar dentin, in predentin.
When discussing this issue, it is necessary to keep in mind that preparing a cavity in a tooth using a drill usually causes a sharp heating of the tooth substance, which is quickly transferred to the internal parts of the tooth. As I. G. Lukomsky points out, excessive pressure with a blunt drill, too long drilling at the same point causes the formation of a large amount of heat, which leads to burns of the processes of odontoblasts and gives sharp pain. And he further emphasizes that “overheating of dentin during drilling is undoubtedly one of the most common factors causing pain.”
Indeed, precise experiments that were carried out by M. Berman measuring the temperature in the tooth cavity when drilling its wall with a bur or when grinding it under a crown showed that the temperature inside the tooth can quickly rise to 60° and higher if a certain processing regime is not followed tooth This overheating of the hard tissues of the tooth causes, as we have already indicated above, a sharp inflammatory reaction from the dental pulp, and in some cases its complete necrosis due to a burn. There is no doubt that the resulting pain may be associated with thermal irritation of the nerve endings embedded in the predentin or in the superficial parts of the pulp. It is difficult to say with certainty whether the processes of odontoblasts play any role in the perception of irritations and their transmission to nerve endings, as many authors suggest. Recent histochemical studies by Avery and Panna showed that Toms fibers throughout their entire length contain a large amount of acetylcholinesterase, which, along with acetylcholine, plays an important role in the transmission of nerve impulses.
The same sharply positive reaction to acetylcholinesterase (AChE) is given by the peripheral zone of the pulp of normal teeth, including the layer of odontoblasts, as well as the adjacent acellular Weil’s layer and a layer rich in cells. These areas of the pulp are known to be rich in nerve fibers and their endings. In the central sections of the pulp, AChE is localized in large nerve trunks that conduct pain impulses from the tooth. It is interesting that in the pulp underlying the area of “dead tracts”, where the dentinal tubules do not contain Thoms fibers, as well as in the area of deposition of secondary or irregular dentin, the reaction to specific AChE becomes negative. Based on these data, Avery and Rapp conclude that Thoms fibers, although not nerve fibers, are capable of conducting impulses from the dentino-enamel junction to the periphery of the pulp, where these impulses are transmitted to the nerve endings. The difficulties associated with the histochemical detection of AChE in dental hard tissues and the possibility of artifacts make further verification and confirmation of Avery and Panna's observations necessary before any conclusions can be drawn from them.
In this regard, the views of the Swedish scientist Brennstrom are of interest, which provide a new explanation for the occurrence of pain during irritation of exposed dentin and the role of protoplasmic processes of odontoblasts in this process. In agreement with the data of Andersen, Karven and Howard, Brennstrom found that irritation of dentin with isotonic solutions of potassium chloride does not cause any pain. However, if this substance comes into contact with the exposed pulp, it will immediately cause severe pain that can last from 15 seconds to 1 minute.
There is no doubt that the occurrence of this pain depends on irritation of the sensitive nerve endings embedded in the pulp at the border with dentin. Since the application of a solution of potassium chloride to exposed dentin did not cause pain, Brennstrom quite logically concludes that dentin does not have nerves. This conclusion is consistent with the above-mentioned results of morphological studies, which could not detect nerves in the composition of calcified dentin.
However, other chemicals, such as concentrated sugar solutions, applied to the surface of exposed dentin are known to cause pain. Painful sensations also occur when the cavity in the dentin is dried for a sufficiently long time by a current of air or when its walls are irritated by a heated metal object. The same effect, according to Brennstrom, is exerted by a rapid change in pressure in the direction of increasing or decreasing it on the surface of exposed dentin. In all these cases, according to the author, there is a change in pressure in the dentinal tubules or a movement of their contents outward, which is accompanied by a massive migration of odontoblast nuclei into the cavity of the dentinal tubules. These fluctuations in hydrodynamic conditions or pressure in the dentinal tubules are transmitted through their contents, i.e., essentially Toms fibers, to the nerve elements of the pulp and, if they are of sufficient intensity, are perceived by them as painful irritations. It is very possible that the same effect can be caused by a change in osmotic pressure in the contents of the dentinal tubules. By this, Brännstrom is inclined to explain the occurrence of pain when exposed dentin is exposed to a concentrated sugar solution.
Thus, unlike previous authors who attributed an active role to Thoms fibers in the perception of pain stimuli, endowing them with the properties of nerve elements, Brännstrom assigns them a much more modest place in the mechanism of pain during dentin irritation. Under the influence of various external factors acting on the surface of exposed dentin, the physical state of Toms fibers changes. These changes in the contents of the dentinal tubules, resulting from drying, changes in pressure, elevated temperature, etc., in turn cause irritation of the nerve endings of the pulp, which, according to Brennstrom, causes the occurrence of pain when dentine is irritated.
The hypothesis expressed by Brännstrom of the occurrence of pain during irritation of dentin, although it requires further detail and clarification, is of undoubted interest and should be taken into account when discussing the issue of dentin sensitivity.
Pulp diseases
Pulpitis most often occurs in acute form. In its chronic form, pulpitis also reveals itself not so rarely. Its signs, of course, are not as pronounced as in acute manifestations and are characterized primarily by susceptibility to thermal irritants - cold and hot food. It is also often accompanied by bad breath. During exacerbations, paroxysmal pain occurs.
Basically, pulpitis according to the classification is gangrenous, fibrous, proliferative. Symptoms that can characterize the presence of chronic fibrous pulpitis can be expressed by pain in response to stimuli of mechanical, chemical and thermal properties. With the latter type, pain occurs upon contact with food that penetrates into the open dental cavity; all this may be accompanied by pulpal bleeding. Chronic gangrenous pulpitis is characterized by the presence of pressure in the tooth with short-term pain from hot food. If the dental cavity is opened, the release of foul-smelling gray matter can be observed. The concremental inflammatory process is characterized by sudden pain, which is caused by:
- vibrations;
- sudden movements;
- by elevator.