Types of tooth extraction
In medical practice, all removal procedures are divided into:
Easy removal
The doctor manages to extract the entire tooth using special forceps; its duration is up to 5 minutes. This is how single-rooted teeth or teeth affected by periodontitis are removed.
Difficult removal
To extract a tooth, the doctor uses auxiliary tools (most often an elevator), and the entire extraction process takes up to 15 minutes. It is most often performed when a part of the root or crown is broken during the removal of multi-rooted teeth.
Atypical removal
It has no clear boundaries in terms of time and extraction method and implies a complex and multi-stage procedure. For this, the doctor can use a bur, an elevator, forceps, a chisel, surgical sutures and needles to close the wound. Often such removal requires from 30 minutes to 2 hours.
This division is reflected both in the cost of the removal itself (due to the various labor costs of the doctor) and in the rehabilitation period:
Simple removal results in minimal damage to surrounding tissue. At the same time, squeezing them with an instrument (and stopping full blood circulation in this area) lasts no more than 5 minutes, and does not in any way affect the subsequent healing of the wound. If you follow the recommendations, the risk of complications is minimal.
Complex removal involves the use of more aggressive instruments and prolonged compression of the walls of the bone alveolus. After it, there may be difficulties with the formation of a blood clot and the development of alveolitis of the “dry socket” type, which is supervised by taking anti-inflammatory drugs and applying turunda with iodoform.
Atypical removal is a surgical intervention in which the doctor violates the integrity of the mucosa, periosteum, or a certain part of the bone. Pressure on tissue can last up to 2 hours, which greatly affects tissue microcirculation. Sometimes a hemostatic sponge is used to stop socket bleeding during such removal. The wound is sutured, which ensures the tightness of the hole and protects it from the development of alveolitis, but it is important to maintain a hygienic regime to avoid infection on the soft tissue.
The doctor’s further tactics, his prescriptions and recommendations for the recovery period depend on how the tooth was removed.
Features of dental position anomalies
Certain anomalies in the position of the teeth are usually grouped together in St. Petersburg under the general term “dental crowding.” If crowding of teeth is registered in a person’s mouth, this makes it significantly more difficult to clean them from plaque, which invariably leads to the development of carious processes. If the teeth are located very closely together, then the contacts between them are not optimal, and the surrounding tissues do not receive the proper level of nutrition and blood supply, which most negatively affects the condition of the gums and bone tissue.
Diastema is the gap observed between the central incisors of the upper dentition. The main reasons may be: a short frenulum on the upper lip, supernumerary teeth, small teeth with significant development of the jaw, and so on.
Narrowing of the dentition is an anomaly in the position of the teeth, characterized by its frequent occurrence. The cause of the narrowing may be diseases of the ENT organs (the baby breathes through the mouth, which is why the upper jaw is underdeveloped), genetic factors and muscle dysfunction. At the moment of narrowing of the dentition, the smile turns out to be narrow, and there are peculiar “buccal corridors”.
Shortening and lengthening of the dentition is observed in most types of malocclusion. The reasons are: bad habits (thumb sucking), muscle dysfunction, mouth breathing. Excessively short or long teeth do not look aesthetically pleasing at all and affect the overall aesthetics of the face. If there is a lengthening of the dentition, the upper lip protrudes forward, and the chin fold deepens. When the dentition is shortened, the lip recedes.
How is tooth extraction performed?
Before removal, the doctor conducts a survey to find out if the patient is allergic to anesthetics and medications. The doctor also asks the patient about the presence of trophic diseases (diabetes mellitus, atherosclerosis) and pathologies of the cardiovascular system (hypertension, arrhythmia, etc.). This is necessary for the correct selection of anesthesia.
Then the doctor administers anesthesia (usually conductive torus for the lower jaw and infiltration for the upper jaw) and waits for the effect to occur.
Simple removal consists of 5 steps:
- applying forceps to the tooth;
- moving them so that the cheeks are under the gum;
- tool fixation;
- luxation (swinging) - necessary to detach the periodontal ligament, which holds the tooth in the bone;
- traction (luxation) - removal of a tooth from the alveolus. This is done by tilting the tooth in the direction of least resistance (where the alveolar wall is thinner) and simultaneously pulling the tooth outward.
For complex extractions, the doctor uses an elevator - a chisel-shaped instrument with a pointed end, which is carefully inserted into the hole and, with its help, pushes the tooth out from the top of the root.
In the process of atypical removal, a surgical field is formed: the doctor dissects the mucous membrane, peels off the flap with the periosteum and removes the bone substance located above the tooth. The tooth itself is removed using an elevator, but often during the removal of wisdom teeth, the doctor is forced to saw it into pieces with a drill, extracting each root and crown separately.
STRUCTURE OF HUMAN TEETH AND PERIODONTAL LIGAMENT
STRUCTURE OF HUMAN TEETH
Teeth (3) are hard, conical organs anchored in the dental alveoli of the jaws.
For greater clarity, the leftmost of the two premolars (molar small teeth) is dissected longitudinally, allowing its internal structure to be examined.
To show the structure of the periodontal ligament, part of the alveolar bone around the right premolar is also removed. Each tooth has a crown (K), protruding from the gum (De), a root (Ko), inserted into the recess of the alveolar bone (AK), and a neck (W), a narrow zone between the crown and the root of the tooth. The neck areas of adjacent teeth are separated from each other by gingival septa (see asterisks). Inside, each tooth has a small cavity - the crown cavity (CC), which is filled with dental pulp (PZ).
Each root has a narrow end - the apex (B), the hole (O) of the root apex, through which blood and lymphatic vessels and nerves pass into the pulp (see arrow).
On a section of the tooth you can distinguish:
• enamel (E), which forms the bulk of the crown and covers the dentin like a cap. The outer surface of the crown has small convexities and depressions called perikymatia (Pk), which correspond to the lines of Retzius (LR) from the inside. Gunter-Schräger lines (GSL) are mainly oriented perpendicular to the enamel surface;
• dentin (D), which limits the tooth cavity;
• cement (C), which completely covers the root and reaches the enamel in the area of the tooth neck.
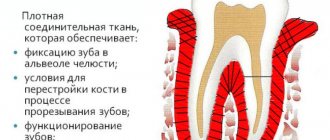
PERIODONTAL LIGAMENT
The collagen fibers of the periodontal ligament, or Sharpey's fibers, are woven into the cementum of the tooth on one side, and into the periosteum and the substance of the alveolar bone on the other.
A narrow space, the periodontal space (PS), separates the roots of the teeth from the alveolar bone. This space is intersected by strong collagen fibers of the periodontal ligament and a number of preelastic, or oxytalan, fibers.
In addition, this space contains a certain amount of loose connective tissue in which lymphatic and blood vessels (CV) are located, and nerve fibers extend from the alveolar bone through its openings.
The periodontal, or alveolodental, ligament consists of elastic collagen fibers, divided into different groups.
At the level of the tooth neck, the following groups of fibers can be distinguished:
• circular (circular) fibers (CF), which surround the neck of the tooth and strengthen the interdental gingival septa (see asterisks) and gingival sulci (DF); • alveolar ridge fibers (AGF), located radially and connecting the periosteum of the alveolar ridge (AG) with the cement of the tooth neck; • transseptal fibers (TV), which connect the necks of adjacent teeth, covered with cement; • dentoperiosteal fibers (DF), connecting the periosteum of the alveoli with the cement of the cervix.
At the level of the roots of the teeth one can distinguish: • horizontal fibers (HF); • oblique fibers (KB), running mainly in an oblique direction relative to the apex of the tooth; • apical (apical) fibers (AF), attaching the root apex to the alveolus.
In reality, the tooth is suspended by the periodontal ligament , which protects the apical blood vessels and nerve fibers from injury during chewing. Because the collagen fibers of the ligament are slightly wavy, very limited tooth movement in the alveolus is possible. Therefore, the alveolodental connection is classified as a type of connection called impaction - gomphosis.
The alveolar bone is covered by the gingiva (De) with the lamina propria (LP) closely adjacent to the periosteum (N). In the area of the floor of the vestibule of the mouth (PO), the gingival epithelium (ED) loses its keratinized layer (C) and transforms into multilayered squamous non-keratinized epithelium (NE) of the cheek (B). The outer surface of the cheek is not shown, but its inner surface is the oral mucosa, consisting of stratified squamous epithelium and the lamina propria (LP), containing mixed buccal glands (BG). Between the skin of the cheek and the mucous membrane there is a layer of striated muscle fibers of the buccal muscle (BM).
Recommendations after removal
Regardless of the method by which the tooth was removed, in the first 2 days the patient must observe a special diet, activity and hygiene. This is necessary to preserve the blood clot in the wound, which helps maintain the sterility of bone tissue and promotes its regeneration.
In the first 48 hours after removal you cannot:
|
Failure to comply with these recommendations most often causes the clot to fall out of the socket and the development of alveolitis or bleeding.
After tooth extraction it is recommended:
- make oral baths from chamomile and sage decoctions (the decoction prepared according to the instructions is taken into the mouth and held there for 10 minutes, without rinsing or moving the tongue) 2-3 times a day;
- take non-steroidal anti-inflammatory drugs (especially after atypical removal, when the tissue is severely damaged and swelling occurs) - nimesulide, diclofenac sodium, ibuprofen, paracetamol, etc. (it is important that the medicine does not reduce blood clotting).
Sometimes patients need preliminary preparation for removal. People taking aspirin and other medications that impair blood clotting should stop taking them a week before the procedure. For those who suffer from increased excitability and anxiety, you can start taking valerian or motherwort 1-2 weeks before removal, having previously agreed with your dentist and your therapist.
Even if the removal was painless and quick, you should not ignore the doctor’s advice. The right approach to rehabilitation will help you avoid complications and recover faster.
Prices for tooth extraction
| Name | Price |
| Consultation | For free |
| Use of bone material | 4,000 rub. |
| Simple tooth extraction | 2,700 rub. |
| Removal of periodontitis tooth | 1,000 rub. |
| Tooth extraction is complicated | 3,200 rub. |
| Removal of a dystopic wisdom tooth | 4,000 rub. |
| Removing a tooth fragment | 500 rub. |
| Removal of exostosis in the area of 1 tooth | 2,500 rub. |
| Removal of cysts and benign formations | 3,500 rub. |
| Treatment of alveolitis | 1,200 rub. |
| Lengthening the clinical crown of a tooth | 5,000 rub. |
| Free flap gum grafting | 8,000 rub. |
| Removing stones from the ducts of the salivary glands | 3,500 rub. |
| Splinting for a jaw fracture | 15,000 rub. |
| Socket curettage | 200 rub. |
| Filling the hole with a medicinal substance (Alvogil, al-vostaz, hemostatic sponge) | 200 rub. |
| Resection of the apex of the tooth root | 4,500 rub. |
| Removing a foreign body from the canal | 1,500 rub. |
Treatment methods
If the anomaly is not accompanied by any aesthetic or functional defects, there is no need for treatment. If specialist intervention is considered necessary, it can be of the following types:
- Orthodontic. Moving teeth into the correct position using removable or fixed orthodontic appliances.
- Surgical. Most often this is the removal of a tooth, which, due to large and complex displacement, is impossible or difficult to move to the desired location.
For example, if it could lead to gum recession or root resorption. In combination with orthodontic methods, compactotomy (bone thinning by drilling) can be used. - Conservative. Grinding of the chewing or cutting surface to adapt to the teeth with antagonists. Filling, restoration of the coronal part.
- Prosthetics. It is used to disguise a clinical crown or an abnormally located tooth under a standard appearance for a given position.
For this purpose, crowns, inlays and onlays are used. In addition to improving aesthetics, prosthetics can be aimed at increasing chewing efficiency by harmonizing occlusal relationships with antagonists . - Combined treatment methods. In particular, compactotomy (surgical method) and subsequent tooth movement (orthodontic stage), or removal and movement.
When drawing up a treatment plan, the doctor selects the optimal protocol to ensure the fullest possible restoration of the functionality and aesthetics of the rows.
Depending on its type, severity, and condition of the teeth, transposition may require any method of solving the problem, ranging from complete non-intervention to removal of one of the transposition units.