July 9, 2020 Last revised: January 12, 2020 Dental diseases
Dental problems affect every person and bring a lot of stress. Most of them occur due to the patient’s fault due to late access to a doctor, but some pathologies appear as a result of unqualified actions of the dentist himself. One of these pathologies is tooth perforation.
Perforation is the formation of a hole in a tooth through which it comes into direct contact with the oral cavity. The hole can form on the wall of the crown, at the bottom of the tooth cavity and on the root. Let's consider all the causes of pathology and methods for eliminating it.
Causes
Perforation of a tooth is simply called a hole. This hole is similar to advanced caries, but often forms for completely different reasons. One of them is the careless actions of the dentist.
In addition to improper actions by the dentist, a hole in the tooth can appear as a result of:
- untreated caries;
- mechanical influence from the outside;
- anatomical features of the jaw shape.
Dentist mistakes
How can improper dentist practices cause a crack or hole in the crown and root? This may occur due to the difficulty in treating the internal structures of the tooth. The obstacles are the branches of the root canals, which make it difficult to access the site of infection. A tooth can also become perforated while increasing the space of the canals with a drill or in preparation for installing a pin.
Perforation of a molar during treatment is accompanied by a sudden pain syndrome and the appearance of blood from the site of the lesion.
Mechanical impact from the outside can provoke a strong blow or careless actions of the dentist while cleaning the dental canals. You need to seek dental help from experienced doctors, read reviews about clinics and give preference to treatment with modern equipment.
An inexperienced dentist may apply force during endodontic correction of a tooth, which will inevitably lead to the appearance of a crack or deep hole. Working with low-quality or outdated instruments can lead to their sudden breakage and getting stuck in the dentin tissue. It is not possible to eliminate pathology without a special microscope. As a result, after a few days the patient’s jaw begins to hurt severely and the periodontal tissue becomes inflamed.
In modern dental clinics, doctors wear special magnifying binocular glasses and use microscopes. This reduces the risk of tissue perforation.
Other reasons
Neglect of the oral cavity and untimely treatment of caries always leads to perforation and even loss of a molar. Complications of caries are dangerous both for the tooth and gum tissue, and for the general health of the patient.
The cause of perforation may be:
- malocclusion;
- tooth damage during sleep;
- wedge-shaped defect;
- demineralization of enamel;
- denture not removed during surgical treatment.
How does a perforated molar hole differ from a carious cavity? When perforation occurs, multiple cracks may form on the surface of the crown. With caries, cracks do not form on the enamel.
Anatomical features of the jaw structure (curved root canals) often prevent thorough sanitation of carious cavities and can cause careless actions by the dentist.
What are the reasons for tooth perforation?
Among the main reasons for the development of pathology, it is worth highlighting the following:
- Features of the structure of the root system. The likelihood of a perforation increases if the dental canals become bent, as the treatment process becomes more complex.
- Injury to a tooth due to impact. In this case, the perforation is a crack.
- Damage to dental tissue by caries. Such processes can lead to thinning of hard tissue and the emergence of a through passage into the tooth cavity or its canal.
In addition, there are a number of reasons that increase the risk of perforation, regardless of the qualifications of the specialist and compliance with the technological process:
- the central axis of the tooth has a deviation towards the cheek, lips or tongue;
- abrasion of tooth tissue, which leads to thinning of its walls;
- when performing therapeutic measures directly through the dental crown.
Symptoms
When should you contact your dentist about suspected perforation? There are indirect and direct symptoms characteristic of this pathology.
Symptoms:
- periodic bleeding from the gums that goes away on its own;
- inflammation of the gums, redness;
- unevenness on the surface of the crown, which can be determined using a tongue or toothpick;
- reactions to changes in food temperature, sweetness and acidity;
- formation of pus in the periodontium, throbbing pain when touched;
- severe pain during dental procedures.
There are also indirect symptoms that may indicate the presence of pathology:
- increased salivation;
- wounds on the tongue while chewing food or resting at night;
- headaches, general weakness, hyperthermia.
Traditional methods of treatment to eliminate perforation are not used. Without dental care, the hole in the tooth will not heal.
Increased salivation and headaches can also appear with other pathologies, but in combination with gum inflammation they suggest a dental disease.
Other causes of perforation
The remaining 5% of clinical cases of sinus perforation injuries occur for the following reasons::
- Not ideal endodontic treatment of tooth canals - the therapist treated the canals, was in a hurry, used excessive force when filling the canal, and under the influence of a rotating canal filler with pressure, the filling material fell beyond the tooth root. We often encounter cases where even fragments of endodontic instruments are sometimes found in the thickness of the filling material, which jam in the canal and tear into pieces, leaving metal fragments in different places of the tooth root;
- Punitive sinus lifting - an inexperienced or rude doctor does not feel the density of the tissues, breaks through the Schneiderian membrane, the bone material is forced into the gap and enters the sinus;
- Author's implantation - it happens that due to the lack of skills in performing a sinus lift and the desire to restore the missing bone, a decision is made - the implant is placed in the residual bone that exists, without bone grafting. Result: the implant completely fails or partially comes out into the sinus.
A fragment of an endodontic instrument in a tooth canal
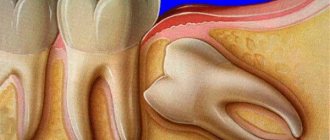
Types of perforations
Violation of tissue integrity appears in the following places:
- on the wall of the crown;
- fundamentally;
- at the bottom of the tooth cavity.
Coronal pathology is the most common, as it is formed due to carious tissue damage. Untreated caries leads to pulpitis - damage to internal tissues and nerves. Pulpitis is characterized by paroxysmal pain in the localized area, which intensifies in the evening and night hours. When treating pulpitis, the root canals are cleaned and the affected pulp is removed.
Damage to the bottom of the tooth cavity occurs when the pins are installed incorrectly in the dental canals. The patient feels pain at the site of the lesion and also notices bleeding. Pathology also appears due to displacement of the tooth axis and active abrasion of the chewing surface.
Damage to the root may not bother a person for a long time, but at this time active destruction of dental tissue occurs.
Perforation of dental roots must be eliminated immediately, otherwise it will lead to inflammation of the connective tissues (periodontal). Also, the cause of root perforation is often their anatomically incorrect structure.
Treatment of tooth root perforation
There are three methods for eliminating perforation - conservative, conservative-surgical and surgical.
- The defect, which is located close to the crown and is clearly visible on an x-ray, is sealed and filled.
- If there is chronic inflammation in the periodontium, it is necessary to make a small incision in the gum to gain access to the hole, remove the infected tissue and seal the cavity.
- Apical damage is corrected only by resection of the root apex.
Diagnostics
Timely detection of perforation and timely elimination of pathology is the best solution to the problem. An undetected hole in a tooth leads to the development of pathology in the tissues or an increase in the size of mechanical damage.
The nature of the pathology can be determined using hardware diagnostics:
- X-ray using a contrast agent;
- vital staining of units;
- electroodontic diagnostics;
- light fluorescence;
- laser diagnostics.
An X-ray with contrast is performed precisely, in 2D format. A targeted X-ray differs from a panoramic X-ray in the small volume of the image - a pair of adjacent units next to the one being examined. In the picture you can see the focus of root inflammation, and also analyze the condition of the sealed canals.
With the help of vital staining of the molar crown, you can see the smallest cracks in the enamel. However, the method does not allow determining deep tissue damage.
Electroodontodiagnosis was used back in Soviet times, when there was no MRI and CT. This method allows you to determine the condition of the pulp after injury or other adverse processes with a molar. The dentist directs the electric current and determines the condition of the internal tissues of the tooth by assessing the excitability of the nerves. Diagnostics answers the questions: is it possible to cure the unit under study, is there a cyst on the root?
Light fluorescence allows you to assess the depth of tissue damage. The method involves illuminating the molars with a special lamp. The diagnostic picture is displayed on the monitor at the same moment. The doctor can see any damage that may be located both in the root system and at the bottom of the tooth, and on the surface of the crown.
Laser diagnostics is carried out using a diode laser with red radiation. This method is the most advanced, as it allows you to detect hidden pathological cavities in hard-to-reach places.
Methods of perforation and torpedoing of wells
After drilling an oil or gas well, its walls are secured with casing pipes; in the intervals of occurrence of productive (oil and gas-bearing) and aquiferous formations, the column is cemented.
In this case, oil- and gas-bearing formations are blocked by casing pipes and a cement ring, and the flow of fluid into such a well is impossible until conditions are created for connecting the productive formation with the well.
To create the possibility of the influx of oil and gas from the formation, a number of channels (holes) are created in the casing and the surrounding cement ring against the oil-bearing (gas-bearing) formation, providing communication between the formation and the well: through these channels, oil and gas enter the well. As a rule, holes in the column and cement ring are created by shooting. This process is called column perforation, and the devices used to shoot through are called perforators.
They are lowered into the well using a logging cable.
Perforation is also used for opening flooded formations in injection wells, for carrying out isolation work and after them: when moving to other horizons, etc. There are 4 methods of perforation: - bullet, - torpedo, - cumulative, - sandblasting. The first 3 methods are carried out in the fields by geophysical parties using the equipment, instruments and equipment at their disposal. Sandblasting perforation is carried out by technical means and oil field services. Bullet perforation. In this case, a firing apparatus consisting of several (8-10) chamber barrels loaded with bullets with a diameter of 12.5 mm is lowered into the hole on an electric cable. The chambers are loaded with explosives and detonators. When an electrical impulse is applied, the bullets pierce the column, cement and are embedded in the rock, forming a channel for the movement of liquid and gas from the formation to the well. Bullet perforators are divided into two types: 1) with horizontal barrels, when the length of the barrels is small and limited by the radial dimensions of the perforator; 2) with vertical barrels with bullet deflectors at the ends to give their flight a direction close to perpendicular to the borehole axis. A rotary hammer with horizontal barrels is assembled from several sections, along which two or four vertical channels and chambers with explosives are drilled. The barrels of the chambers are loaded with bullets and sealed with sealing gaskets. The upper section has two igniters. When current is supplied through the cable, the first ignition device is triggered, and detonation spreads along a vertical channel to all chambers crossed by this channel. As a result of the almost instantaneous combustion of the explosive, the gas pressure in the chamber reaches 2000 MPa, after which the bullet is ejected. An almost simultaneous shot occurs from half of all barrels. If it is necessary to double the number of shots, a second pulse is sent along the second cable core. In this case, the second half of the barrels from the second ignition device is triggered. In a hammer drill, the mass of the explosive charge in one chamber is insignificant (equal to 4-5 g), so its penetration capacity is low. The length of the resulting perforation channels is 65-145 mm (depending on the properties of the rock and the type of perforator), the diameter of the channel is 12.5 mm. The figure shows a bullet perforator with vertically curved barrels PVN-90. With a vertical arrangement of trunks, the volume of chambers and the length of the trunks are greater than with a horizontal arrangement. In each section, two barrels are directed upward and this compensates for the reactive forces acting on the hammer drill at the time of the shot. One chamber transfers explosion energy to two barrels at once. The mass of explosives in one chamber reaches 90 g. The gas pressure in the chambers is 600-800 MPa. The effect of gases is longer than with a horizontal arrangement of trunks. This allows you to increase the initial speed of the bullet and the penetration ability of the hammer drill. The length of the perforation channels in the rock is 145-350 mm with a diameter of about 20 mm. Each section of the perforator has four vertical shafts, at the ends of which smooth deflector grooves are made. Bullets made of alloy steel are coated with copper or lead to reduce friction in the deflectors. A shot from all barrels occurs almost simultaneously, since all chambers with explosives are connected by a fire channel. Torpedo perforation is carried out by devices lowered on a cable, and differs from bullet perforation in that an explosive projectile equipped with a delayed-action fuse is used for firing. The mass of the internal explosive charge of one projectile is 5 g. The device consists of sections, each of which has two horizontal barrels. The projectile is equipped with a filament-type detonator. When the projectile stops, the internal charge explodes, resulting in cracking of the surrounding rock. The explosive mass of one chamber is 27 g. The depth of the channels, according to test results, is 100-160 mm, the diameter of the channel is 22 mm. Per 1 m of filter length, usually no more than four holes are punched, since torpedo perforation often causes destruction of casing columns. Cumulative perforation is carried out by firing perforators that do not have bullets or shells. Penetration of an obstacle is achieved through a focused explosion. This focusing is due to the conical shape of the surface of the explosive charge, lined with a thin metal coating (copper sheet 0.6 mm thick). The energy of the explosion in the form of a thin beam of gases - lining products - pierces the channel. The cumulative jet acquires a speed at the head of up to 6-8 km/s and creates a pressure on the obstacle of (0.15-0.3) 106 MPa. When fired, a narrow perforation channel with a depth of up to 350 mm and a diameter in the middle part of 8-14 mm is formed in the obstacle. The dimensions of the channels depend on the strength of the rock and the type of hammer. Cumulative hammer drills are divided into framed and frameless (belt). Box hammer drills are reused many times after they are recharged. Unframed - disposable. Perforators are lowered on cable (there are small-sized perforators lowered through tubing), as well as on tubing. In the latter case, the explosion is initiated not by an electrical impulse, but by dropping a rubber ball into the tubing, which acts like a piston on the explosive device. The mass of explosives of one shaped charge (depending on the type of hammer drill) is 25-50 g. The use of hammer drills of various types and designs depends on the density of the rocks being opened. It is recommended to use cumulative perforation in hard rocks, projectile perforation in less dense and low-permeability rocks, and bullet perforation in loose rocks and weakly cemented sandstones. The maximum thickness of the interval opened by a cumulative perforator reaches 30 m, torpedo - 1 m, bullet - up to 2.5 m. This is one of the reasons for the widespread use of cumulative perforators. Belt perforators are much lighter than casing ones, however, their use is limited by the pressure and temperature at the bottom of the well, since their explosive cartridge and detonating cord are in direct contact with the well fluid. In such hammer drills, the charges are mounted in glass (or other material) sealed cups, which are placed in the holes of a long steel belt with a weight at the end. The entire garland descends on a cable. Usually, when fired, the tape is not completely destroyed, but it is not used for reuse. After shooting, the head, weight, and tape are removed to the surface along with the cable. The disadvantages of frameless rotary hammers include the inability to control the number of failures, whereas in cased ones such control can be easily accomplished by inspecting the casing removed from the well. Cumulative hammer drills are the most common. By selecting the necessary explosives, it is possible to regulate their heat resistance and pressure sensitivity over wide ranges, thereby expanding the possibilities of perforation in wells with abnormally high temperatures and pressures. Hydrosandjet perforation is based on the use of the abrasive and jetting action of a jet of liquid (water, oil) with sand suspended in it, coming out under high pressure from a narrow hole (nozzle). Within a few minutes, such a jet creates a deep channel in the casing, cement ring and rock, providing reliable communication between the well and the formation. The device is lowered into the well using pump and compressor pipes, through which liquid and sand are supplied under high pressure. Flowing from the nozzles at a high speed, reaching several hundred meters per second, the liquid with sand breaks through the production casing, the cement ring and penetrates into the rock to a depth of 1 m. During the perforation process, under the influence of an abrasive jet of liquid (up or down along the wellbore), it can a slot channel will form or (with circular rotation of the jet) the column will be cut off along the ring, which is necessary, for example, to remove part of the casing. Torpedoing in a well is an explosion produced using a torpedo (explosive charge). In addition to the explosive charge, the torpedo contains means for the explosion: a fuse consisting of an electric fuse and an explosion-sensitive detonator capsule, and a block of explosive that amplifies the initial detonation impulse. It is lowered into the well on a logging cable, the core of which is used to activate the fuse and the entire torpedo charge. Torpedoing is used to destroy the rocks of productive formations - the formation of cracks in them for better oil or gas recovery, as well as for the purpose of breaking or shaking stuck drilling, casing and tubing pipes, crushing metal objects at the bottom of the well (cones, bits, etc. .). Sometimes torpedoing is used to remove sand plugs formed in the wellbore, clear the bottom-hole zone of clay sediments, clean the filter, break through a window in the casing for drilling a new shaft, etc.
Therapy
Prompt treatment of perforation can save the unit from complete destruction. The doctor chooses a treatment method depending on how long ago the pathology appeared and the location of the disease.
First, the suspected site of the lesion is examined, then the patient is sent for a tomogram or x-ray. Before eliminating the pathological cavity, a thorough treatment of the tooth is carried out, including the removal of tartar and plaque. They also treat inflammatory foci on the mucous membranes (stomatitis, etc.).
The dentist is obliged to find out important information from the patient: about food preferences and nutritional patterns, about careful hygiene, about dental diseases in the past. This information forms the medical history necessary for an accurate diagnosis and choice of treatment method.
The doctor should also check for the presence of implants in the patient’s mouth. If some implants are outdated or faulty, they need to be replaced. Old fillings installed in the oral cavity also require replacement.
Closing a pathological cavity is similar to a conventional filling. The dentist numbs the gums with injections, isolates the molar with cotton swabs and cleans the problematic canals with a drill. After the necessary disinfecting manipulations, the pathological cavity is closed with filling material.
Tooth perforation during canal cleaning
If perforation occurs directly during endodontics, the following must be done:
- stop bleeding in the mouth;
- carry out sanitation of the affected area;
- cover the crown with temporary filling material;
- give the patient pain medication;
- prescribe a course of antibiotics.
In case of perforation, a molar can be saved if the pathology is treated in a timely manner.
After closing the cavity with temporary fillings, further treatment is carried out: cleaning the canals and installing a permanent filling. The quality of the filling is checked using an x-ray. However, definitive crown restoration does not guarantee long-lasting treatment results, and the patient should visit the dentist regularly for check-ups (at least twice a year).
If there is no access to the root canals in the usual way, the dentist makes an incision in the gum. After the necessary manipulations with the canals and installation of the filling, the gum is sutured.
In case of serious damage to a significant part of the unit, surgery is performed: replantation, root resection. If the tooth cannot be saved, it is removed and then an implant is installed. Perforations no larger than 1 mm in size respond well to treatment; otherwise, the result will depend on many reasons: how old the pathology is, the presence of a focus of inflammation, and other characteristics.
Root resection is carried out with a special dental drill (the apical section is subject to amputation), the infected area is sanitized with antisetics. The gum mucosa of the affected area is excised, sutured and disinfected.
Tooth perforation - where and how does it occur?
Depending on the location, the holes are divided into several types of perforation:
- at the bottom of the tooth cavity;
- in the side wall;
- at the root of the tooth.
The most common type of perforation occurs in the coronal part of the tooth. This occurs as a result of prolonged neglect of the dentist or incomplete treatment. Caries affects the tooth tissues deeper and deeper, softening and destroying them until the wall is depleted and a perforation is formed.
Tooth perforation
Another reason may be mechanical stress. As a result, a crack appears in the tooth. And the reason for this may be not only a strong blow, but also unskilled actions of the dentist when trying to install the pin with significant force.
The occurrence of perforation can be facilitated by the anatomical features of the patient’s tooth roots. The doctor may not be able to see the bends on a poor-quality x-ray and, when cleaning or expanding the canals, violate its integrity. If tooth perforation occurs during a dental appointment, you will feel it immediately. A sharp acute pain will not allow you to miss this moment. And the doctor should see characteristic signs - the appearance of bleeding from the formed hole.
What is tooth perforation
A qualified specialist can and should correct this situation on the spot by filling the defect. But here one small condition arises, 1-1.5 mm in size. If the resulting hole is larger, then through it the filling material can go beyond the boundaries of the tooth and cause many problems, including periodontitis.
Perforation of one of the roots during endodontics is no less dangerous. This happens in most cases due to violation of the rules and techniques of working as a dentist. It makes no sense to figure out later why this happened, since there is a long work ahead to save the tooth. In this case, sitting in a chair, you will feel a stabbing pain, and the dentist will see blood appearing in the canal. These symptoms make it clear that there is a problem and it needs to be solved.
A tooth root perforation is a hole in the root of a tooth.
There are cases when tooth perforation was not detected in a timely manner. In such situations, suspicion can be caused by constant aching pain and an inflammatory process in the gums in the area of the damaged tooth. An X-ray examination will help confirm the final diagnosis.
Replantation
This dental procedure involves gently removing a tooth and then returning it to its place. Replantation is often carried out when healthy units fall out for some reason (trauma, loosening). The tooth returned to the socket is fixed using a special splint.
If a healthy tooth falls out of its socket, it is necessary to place it in saline solution and visit the dentist as soon as possible.
The molar removed from the socket is processed and treated on the surgical table, and then returned to its place. The tooth does not take root immediately; sometimes it takes 6-12 months to adapt. And even after complete engraftment, the replanted unit will not be able to efficiently perform its chewing functions, and also becomes unsuitable for the installation of ceramic crowns and other implants.
Contraindications for replantation:
- cardiovascular pathologies;
- blood diseases;
- mental illness;
- total destruction of the molar;
- malignant neoplasms.
The tooth takes root well with an intact crown and root. However, the quality of chewing function is significantly influenced by the preservation of the dental nerve: the unit will last another 12-14 years. When the nerve is removed, the functionality of the molar decreases. The implanted tooth is able to withstand the usual chewing load only 6 months after installation; before that, care should be taken when chewing food.
At first, it is recommended to chew on one side and treat the oral cavity with antibacterial agents as prescribed by the dentist. In order for the molar to take root well, they take medications with calcium and vitamin D. If the gums and cheeks are swollen after implantation, you need to apply a cold (but not ice) compress.
Also, during the rehabilitation period, heavy physical activity, sudden changes in temperature (sauna, steam room, cold/hot drinks), smoking and alcohol consumption should be completely eliminated. To speed up tissue healing, it is recommended to visit a physiotherapy office. When prescribing antibiotics and analgesics, you should strictly follow the dosage regimen and not interrupt the course at your own discretion.
Removal of a tooth
In what cases is removal of a perforated molar indicated? This is an extreme measure, which is resorted to in exceptional cases:
- severe root destruction;
- periodontal damage due to severe tooth mobility;
- extensive purulent focus of inflammation;
- anatomical features of the jaw structure.
However, even after the molar is removed, treatment continues, but at home. For this purpose, medications are prescribed to restore tissue after inflammatory processes, antiseptics for mouth rinsing, and anti-inflammatory ointments.
Removal of a perforated molar is associated with serious pathologies in the jaw bone tissue. Sometimes recovery processes last for several months in a row. Until the functionality of the jaw bone is completely restored, it is prohibited to install implants or perform prosthetics. Only after complete healing and restoration of the affected tissues can orthodontic procedures be carried out, this also applies to the installation of braces.
Old perforations that occur after tooth extraction or therapeutic treatment
If perforation was not detected after tooth extraction, the patient may attribute the discomfort to the consequences of surgery. It is worth saying that after a couple of weeks the stage of acute pain passes, and in the area of the resulting defect in the maxillary sinus, a so-called fistula appears, which connects the surface of the gum to the sinus.
This process is accompanied by symptoms characteristic of chronic sinusitis; among other things, patients complain of pain, purulent discharge from the nasal cavity, and swelling of the cheek. Treatment consists of the use of therapy aimed at stopping the inflammatory process and surgical methods that eliminate foreign bodies in the maxillary sinus.
If we summarize the above, we can say that the removal of teeth in the upper jaw, as well as their treatment, should be carried out as competently as possible. Perforation of the maxillary sinus can have quite serious consequences for the patient’s body. In some cases, long-term hospital treatment is required. The addition of an infectious process is especially dangerous.
Such a complication can be avoided if the dentist is sufficiently competent, who must take into account the anatomical position of the teeth and the maxillary sinus before performing any complex dental procedures related to the upper jaw. Based on this, the dentist is obliged to highlight all the anatomical and topographical features of the patient and conduct qualified treatment.
Before the procedure for removing, implanting or treating upper teeth, the doctor must take a targeted photo, which will help visualize the area with which he will be working. If these conditions are met, such a serious complication as perforation of the maxillary sinus can be avoided.
Complications
With any treatment, complications are possible that cannot always be prevented or foreseen. This is due to the structural features of the body’s tissues and the reaction to intervention.
Complications:
- spread of infection to the periosteum;
- insufficient cleaning of the channels;
- periodontitis;
- a fragment of the removed root remained.
The listed complications can lead to diseases: granuloma, inflammation of the periosteum, cyst, crowding of teeth, molar loss.
Periodontitis is an inflammation of the tissues around the treated tooth. In mild cases, this will lead to the formation of a fistula: the pus needs to come out somewhere. In severe cases, the periosteum may be damaged, so the molar is simply removed to avoid the spread of infection.
The formation of a cyst is an attempt by the body to isolate the source of infection within the tissues. However, the cyst tends to increase in size, which can lead to the most undesirable consequences and the spread of infection to nearby healthy tissue. The cyst is removed along with the pathological tooth, there is no other way out.
After root resection or elimination of pathology at the bottom of the dental cavity, the cheek may swell. This does not refer to any type of disease, but is treated with a cool compress on the cheek. However, if your cheek is very swollen, you need to call the dentist and report what happened (pick up the phone immediately after treatment). It is unacceptable to apply ice compresses to the cheek: you can severely chill the dental nerves.
What is this pathology?
When this type of problem occurs, a hole is formed between the cavity and the root canals with tissue. This problem can arise due to mechanical damage to the tooth during an injury, in the event of a medical error during treatment, as well as in advanced caries.
Perforation (perforation) occurs in the following places:
- in the area of the bottom of the dental cavity;
- in the root system;
- in the walls of the tooth.
may also occur after tooth extraction .
There are two types of perforation depending on the duration of their formation:
- fresh – treatable immediately after its detection;
- neglected - the tissues have been injured for quite a long time, which led to the development of infection.
Prevention
You should follow a proper diet and take good oral care at home.
- Cleansing the oral cavity should be done in the morning and before bed; during the day after eating, it is recommended to rinse your mouth with plain water or dental elixirs.
- Instead of a toothbrush, it is recommended to use an irrigator to cleanse the oral cavity. This is especially true for gum inflammation. The irrigator cleans teeth and interdental spaces using a stream of water under pressure. This is a painless and modern method of oral care. Instead of plain water, you can use herbal solutions.
- The diet must be carefully reviewed. The emphasis is towards reducing sweets, baked goods and solid foods. The menu should include fresh and boiled fruits/vegetables, dietary meats, and herbs.
- Dentists advise quitting smoking and drinking alcohol.
- Stop engaging in traumatic sports (martial arts, extreme sports) to minimize the possibility of jaw injury.
- Do not neglect routine dental examinations, which are recommended every six months.
Otherwise, tooth perforation does not depend on the patient. You need to choose trusted clinics and professional dentists to treat caries and other diseases.