March 10, 2020 Last revised: September 12, 2020 Bite correction
A beautiful smile and straight teeth are the calling card of any person. But not all parents know that they need to take care of their child’s beautiful smile already during the formation of baby teeth. How does the primary occlusion affect the formation of the dental system, and what effect does it have on permanent teeth? The article describes the difference between primary and adult occlusions and methods for correcting dental defects.
Forms of occlusion
Dental occlusion can be static or dynamic. Static occlusion is assessed when the jaw is at rest and the upper and lower teeth are closed. Dynamic occlusion is assessed as the patient performs chewing movements.
Types of bite and causes of pathological changes
If the upper teeth protrude in front of the lower teeth, an orthognathic bite is diagnosed. The main reasons for the development of pathology: prolonged finger sucking or use of pacifiers in childhood.
More serious changes in bite can be caused by:
- difference in size of the upper and lower jaws;
- hereditary factors;
- partial absence of teeth;
- cleft palate;
- different sizes of opposing teeth;
- displacement of the jaw joint after injury;
- poorly fitted crowns, braces.
Orthognathic bite, on the contrary, provokes protrusion of the upper lip and smoothing of the nasolabial grooves. If there are obvious deviations, the patient receives a referral to an orthopedist. Anthropometric data is not enough to accurately determine the height of the bite and manufacture braces or dentures.
Anatomical and physiological method
The specialist takes measurements and applies the golden ratio formula. The doctor can make an impression, a wax model of the jaw. When taking measurements, special occlusal rollers are used. The method is considered obsolete because there is a high probability of errors in the calculations.
The physician may inadvertently underestimate or overestimate the measurement results. As a result, the manufactured prosthesis will dangle or, conversely, put pressure on the jaw.
You can quickly check for malocclusion using tracing paper. Remains of paint on the enamel will show exactly where the teeth touch, but will not be able to assess the force of jaw closure.
Despite the inaccuracy, the dentist can use the simplest anatomical and anatomical-physiological methods before determining the bite during prosthetics using modern technologies.
Digital method
In modern dentistry, the height of the bite (the distance between the upper and lower jaw) is determined using digital technology. The most common occlusal analysis system is the T-Scan system. The patient needs to bite on a special thin sensor block. The computer program will not only analyze the bite, but also measure the pressure between the opposing teeth.
Special software will calculate the load on each incisor and molar and check the trajectory of the jaw movement during conversation, chewing or at rest. T-Scan also provides an animated digital image of the dentition.
An examination using a digital sensor is also carried out after the completion of the prosthetic and implantation procedure. The clinician can ensure that the bite height in the centric occlusion is balanced. The T-Scan system significantly increases the effectiveness of orthopedic and orthodontic procedures. The patient will not need to return to the clinic to have the dentures adjusted.
Reviews
The formation of a permanent bite is a complex multi-stage process, the correctness of which is determined by many factors.
Its anomalies distort not only external aesthetics, but also complicate the work of many internal organs and their systems.
Orthodontic dentistry today offers several options for solving this problem for each patient.
You can share interesting and important information on this topic and express your opinion on the effectiveness of a particular treatment method by leaving a comment on this article.
If you find an error, please select a piece of text and press Ctrl+Enter.
Tags permanent bite bite
Did you like the article? stay tuned
Planning for prosthetics
Before starting the procedure for manufacturing and installing a prosthesis, the specialist conducts an examination and asks:
- orthopantogram;
- TRG image in lateral projection;
- spot x-ray.
If the installation of a partial denture is planned, the condition of the supporting molars is additionally assessed. Next, the specialist can take a “before the procedure” photo. Using a special program, a 3D model of the jaw is built.
In a dental laboratory, a prosthesis is designed using virtual templates. The computer program calculates reference points and bite height.
If prosthetics on implants is planned, the condition of the jaw bone is additionally assessed and the installation depth of the titanium rod is calculated. To avoid errors, the finished prosthesis is not made by hand, but using CAD/CAM technology. Thanks to a fully automated planning and manufacturing process, dental restorations restore normal occlusion.
Prevention of pathologies of permanent occlusion
To avoid problems in a child, parents need to:
- take a responsible approach to pregnancy planning, pregnancy and choose a rational route of delivery;
- accustom the child to eating solid food in a timely manner;
- monitor oral hygiene;
- prevent the formation of bad habits;
- promote the formation of correct posture and normal anatomical position during sleep;
- Make regular preventive visits to the pediatric dentist.
4.3.3. Types of bite
Bite
called the type of closure of the dentition in central occlusion.
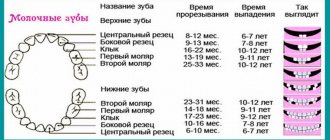
Throughout a person's life, teeth go through two generations. By the age of two years, a temporary bite is formed.
The number of teeth in a temporary dentition is normally 20. According to group affiliation, they are represented by incisors, canines and molars.
At about six years of age, the first permanent teeth appear. The first permanent molars erupt behind the second temporary molars. From this moment until the complete replacement of temporary (baby) teeth with permanent ones, it is customary to call it a removable bite.
The number of teeth during this period varies.
This usually occurs before age 14. If there are no milk teeth in the oral cavity and only permanent teeth are present, the bite is called permanent.
Normally, the number of permanent teeth in a person in a permanent dentition is 28 – 32. According to group affiliation, these are: incisors, canines, premolars and molars.
DIFFERENCES IN TEMPORARY AND PERMANENT TEETH
⇐ PreviousPage 2 of 13Next ⇒| Signs | Features of temporary bite | Features of permanent bite |
| 1. Number of teeth. | 28 — 32 | |
| 2. Group affiliation. | Incisors, canines, molars. | Incisors, canines, premolars, molars. |
| 3.Size of crowns. | Less. | More. |
| 4.Ratio of width and height. | Width prevails. | Height predominates. |
| 5. Color. | White - blue. | White - yellowish. |
| 6. Transition of the crown to the neck. | Sharp, due to the enamel roller. | Smooth. |
| 7. The widest part of the crown | Cervical. | Equatorial. |
| 8. Retention points. | The fissures are shallow, there are no pits. | The fissures and pits are deep. |
| 9. Expressiveness of crown tubercles. | After 4 years they are normally erased. | Normally, they do not wear off in childhood. |
| 10. Location of teeth in the dentition. | In periods 1 and 2, the temporary occlusion is dense; in period 3, tremors appear (after 3 years). | Normally without trema or diastema. |
| 11. Mobility of teeth. | During the period of physiological resorption it increases. | Normally absent. |
| 12. Location of roots. | In single-rooted plants there is a pronounced vestibular bend. In multi-rooted plants, the roots diverge widely. | The sign of root angle is expressed. |
| 13. Size of the tooth cavity. | Relatively large, wide root canals. | Relatively large after eruption, the width of the root canals varies; with age, the tooth cavity decreases, the root canals narrow. |
| 14. Thickness of hard tooth tissues. | Smaller. | Big. |
| 15. Degree of mineralization. | Smaller. | Big. |
| 16. Presence of immune zones of enamel. | None. | Expressed in the area of tubercles and cutting edges. |
| 17. Structure of dentinal canals. | Short, wide. | Already, longer, with anastomoses. |
V. SCHEME OF OOD - DIAGNOSIS OF CARIES IN CHILDREN.
The task of the action is to identify the symptom complex and correlate it with the known description of the disease.
| Diagnostic stages | Survey facilities and conditions | Criteria and forms of Self-Control |
| A | B | IN |
| I. Complaints of the patient a) about the appearance of white spots on the teeth b) about pain from sweet, sour c) from cold, hot d) about food ingestion e) about tooth decay | Calm atmosphere, gentle treatment of the child Sometimes the child himself shows a bad tooth | There may be no complaints with initial forms of caries with initial caries (caries in the spot stage) with medium caries, pain is possible insignificant with superficial caries with deep caries with medium and deep caries |
| P. ANAMNESIS 1. Life of the child ANTENATAL PERIOD State of health of the mother The course of pregnancy in the mother: toxicosis, hypovitaminosis, hypoxia, anemia, infectious diseases, etc. Weight of the child at birth, full term POSTNATAL PERIOD a) nature of feeding b) diseases of the child, especially in the first year of life: dyspepsia, rickets, hypovitaminosis, allergic conditions, infectious diseases, etc. c) chronic diseases: rheumatism, chronic tonsillitis, chronic kidney diseases, lungs, etc. during the period of teeth formation after the formation of teeth d) the presence of caries in parents (hereditary factor) f) the nature of nutrition: - is the child’s food varied, does he eat dairy products, fish, fruits, vegetables, cereals - what is the consistency of the food consumed - is he actively Does the child chew - does he consume a lot of carbohydrates in the form of sweets: cookies, gingerbread, candy e) oral hygiene: since when does he brush, with what, how many times, with what brush? How does your family feel about oral hygiene? | Information provided by the mother, extract from the child’s outpatient card | Children born to mothers suffering from extragenital diseases are susceptible to early and increased susceptibility to caries. In the presence of these factors, the mineralization of the crowns of temporary teeth is disrupted; after eruption, teeth become more susceptible to caries. In premature children with low body weight, caries develops more often. Artificial feeding can contribute to the development of caries. Affects the mineralization of permanent teeth, makes them susceptible to caries - can disrupt the mineralization of permanent teeth - contributes to the appearance of white carious spots in the cervical region of various groups of permanent teeth is a predisposing factor for the development multiple caries in a child, good nutrition contributes to the formation of caries-resistant teeth; soft food contributes to the rapid formation of dental plaque with “laziness in chewing”; self-cleaning of the oral cavity worsens; contributes to the development of a cariogenic situation in the oral cavity; low level of oral hygiene contributes to the development of caries |
| III. History of the disease: when did parents first notice a change in the shape and color of teeth? When did you first go to the dentist? | ||
| IV. Objective examination: a) appearance of the child, condition of the skin, type of breathing b) condition of the lymph nodes: submandibular, cervical, mental c) salivary glands: amount and rate of salivation, amount and nature of saliva, d) mucous membrane of the mouth, pharynx, tonsils e ) filling out a dental formula e) examination of hard tooth tissues (carious lesions) ENAMEL presence of a stain presence of a stain DENTIN presence of a cavity | external examination palpation of lymph nodes examination using a mirror examination using a mirror examination using a mirror and probe compare with a healthy tooth probing probing probing | Children of poor nutrition, asthenic build with pale skin often suffer from multiple caries; full, loose, hypersthenic type children (with a predominance of carbohydrate foods) have a predisposition to the development of caries; mouth breathing favors the development of caries; enlarged lymph nodes are palpated in chronic diseases and multiple complicated caries; hyposalivation and increased viscosity saliva contributes to the development of the carious process; a chronic inflammatory process in the tonsils contributes to the development of multiple caries; these diseases mutually determine each other; identification of carious teeth; carious spots are usually white, less often pigmented; the surface is smooth; roughness is determined in the case of the transition of the spot into superficial caries; in superficial caries; the surface of the spot is rough; medium caries cavity within the upper layers of dentin, pain in the area of the enamel-dentin border with deep caries within the deep layers of dentin, pain in the bottom of the cavity |
| IN TEMPORARY TEETH AND TEETH WITH AN IMFORMED ROOT SYSTEM, DEEP CARIES IS PRACTICALLY NOT ENCOUNTERED, DEEP DESTRUCTION OF DENTIN DUE TO THE MORPHOFUNCTIONAL FEATURES OF DENTIN AND PULP IS ALWAYS ACCOMPANIED BY STRONG REACTION NEW AND DYSTROPHIC CHANGES IN THE PULP. | ||
| Condition of the dentin g) type of carious cavity h) number of affected teeth i) what is the location of the cavities smooth surfaces of the incisors of the upper and lower jaw chewing surfaces contact surfaces cervical region lingual surface j) which groups of teeth are affected | probing | in the acute course of caries - light, moist, easily removed in layers, can fill a large volume of the carious cavity, which is why the cavity seems shallow; in the chronic course of caries - pigmented, dry, dense, the edges of the cavity in the acute course are sharp, easily break off, the development of a cavity is characteristic along the plane; in a chronic course, the edges of the cavity are rounded, undermined, depending on the average index of caries intensity in a given area, three degrees of caries activity are distinguished: a) compensated b) subcompensated c) decompensated are affected in children under 2.5 years of age (due to unfavorable antenatal calcification) in temporary molars are affected in children after 3 years of age, in permanent teeth, due to the accumulation of dental plaque in places of incomplete mineralization (fissures) in temporary molars, in children aged 4 years, in permanent teeth, due to the accumulation of dental plaque in places of incomplete mineralization, it is often affected in permanent teeth, due to accumulation of dental plaque in places of incomplete mineralization in temporary teeth, especially in acute cases, circular caries is often found, rarely affected, sometimes with an atypical course of caries (in children with diseases of the central nervous system), the incisors on the lower jaw are affected by decompensated caries |
| Make a preliminary diagnosis in accordance with the classification | ||
| V. Additional examination 1. Vital staining 2. Fluorescent stomatoscopy 3. Dental X-ray (rarely used) 4. Refer the child to other specialists (for decompensated caries) | 2% methylene blue solution, before staining, soft plaque is removed, the tooth is isolated from saliva, after which the paint is applied for 2-3 minutes. if there is a special office if there is a special office children's clinic | a carious spot is well stained; a decrease in the luminescence of a carious spot against the background of a gentle light green glow of healthy hard tissues; hidden carious cavities are revealed; chronic diseases are revealed |
| VI. Carry out differential diagnosis. | ||
| Diseases with a similar clinical picture | Signs not typical for caries | |
| 1. Hypoplasia 2. Fluorosis 3. Chronic gangrenous pulpitis 4. Chronic periodontitis 6. Chronic fibrous pulpitis | a) teeth of the same period of formation are affected b) symmetrical teeth of the same period of development have the same defects c) aniline dyes do not stain stains a) teeth of the same period of formation or a large group of teeth are affected b) there may be the same or different elements (stains, erosions, mottling ) in different areas of the crowns c) aniline dyes do not stain stains a) the tooth was sometimes sick in the past b) pain in the depths of the tooth cavity or in the canal c) destruction of bone tissue in the area of bifurcation of the roots of primary teeth and in the area of the root apexes is often detected by x-rays a) the tooth often hurt in the past b) always - destructive changes in the periapical tissues, detected x-ray c) change in tooth color a) pain and bleeding when probing at one point of the bottom of the carious cavity | |
| Make a final diagnosis: a) type of pathology - dental caries b) form of caries - compensated, subcompensated, decompensated c) stage of caries: spot, superficial, medium, deep |
Plan for comprehensive sanitation of the oral cavity.
1. Teach your child to brush their teeth properly
a) toothbrush (taking into account the degree of hardness)
b) toothpaste (hygienic or therapeutic and prophylactic)
2. Teach parents to control teeth brushing at home
- treatment of tooth surfaces with 2.5% tincture of iodine - well-cleaned tooth surfaces will be light (plaque will turn brown)
3. Fill carious cavities, restore contact. points
- normalization of the act of chewing, prevention of gum injury when chewing.
4. Refer the child for orthodontic treatment (if indicated)
-correction of dental anomalies and deformations normalizes the act of chewing and the uniform load of periodontal tissues.
5. Removal of supragingival dental plaque
-smooth surface of teeth after removal.
6. Removal of subgingival dental plaque
-surface of enamel or cement within the periodontal pocket during inspection
7. Refer the child for frenuloplasty, correction of the vestibule of the mouth (if indicated)
-prevention of the atrophic process in the gums and periodontium.
Nutrition
It is necessary to pay attention to the frequency of meals and distribution within 24 hours; frequency and amount of consumption of sugar and other easily fermentable carbohydrates; consistency of food, its saturation with fluorides, drawing the attention of the patient’s parents to the role that these factors play in the risk of developing caries.
So, for example, if the amount of carbohydrates consumed by a child during the day corresponds to age standards, we can talk about a low risk of developing caries for this factor. But one of the key points in assessing risk is the frequency of consumption of sweets. Even a small snack - a cake or candy - in the intervals between main meals contributes to the production of acids. Therefore, the risk of developing caries increases.
A low frequency of meals per day (maximum 5, including snacks) also corresponds to a low risk of developing caries. Increasing the frequency of doses to 7 or more entails a significant increase in risk.
Interestingly, children's nutrition depends significantly on cultural factors including social and family norms. If the patient's parents and the doctor belong to different social groups, then the doctor's recommendations regarding changes in family eating habits are often ignored (often this concerns night drinking and eating). However, despite the fact that parents’ knowledge about the benefits of rational nutrition for children is rarely materialized in practice, it should be constantly updated in conversations held during clinical examinations. It is optimal if dental education and motivation to care for the oral cavity of children and limit sugar in their diet begins during pregnancy. As a result of such work carried out with expectant and young parents, it is possible to achieve a reduction in the increase in caries of primary teeth in children by up to 86% in physiological pregnancy and 78% in complicated pregnancy.
Sanitary education work is an integral part of the basic program for the prevention of children at risk of developing caries.
Oral hygiene
Numerous Russian and foreign literature sources indicate the need to care for children's teeth from the moment they appear . Caring for infants' teeth consists of removing dental plaque using both finger brushes and gauze swabs generously moistened with boiled water. The quality of this procedure is of particular importance. Destroying dental plaque at least once a day is more effective than the habit of repeated brushing. It is believed that the first teeth should also be brushed twice a day, and after the eruption of temporary molars, a minimum of toothpaste should be added to the toothbrush; the paste should not contain fluoride due to the possibility of it being swallowed by the baby, since excessive consumption of fluoride during the period of tooth formation is considered one of the reasons development of fluorosis. This opinion is not supported by all authors. Currently, when the prevalence and intensity of caries in young children have begun to grow catastrophically, the use of fluoride-containing pastes is considered not only desirable, but also necessary due to their proven effect on caries reduction. At the same time, there was a decrease in the permeability of white carious spots by 36.2%, a decrease in their size by 23.7%, a decrease in the electrical conductivity of areas of focal demineralization by 45.5%, and an increase in the rate of enamel remineralization by 13.1%. The increase in caries intensity decreased by 1.82.
It is advisable to use toothpastes with a fluoride concentration of 500-550 ppm , since the use of toothpastes with a lower concentration of fluorides or their absence is ineffective. In children with a high risk of developing caries, it is necessary to use a more concentrated fluoride-containing paste (1000-1100 ppm) . There are no special children's toothpastes containing more than 550 ppm fluoride in our country yet. However, there are gels “Just for kids” (with 0.4% tin fluoride) and “Stangard”, which are recommended to be used after traditional teeth brushing, once, at night, applied to cleaned surfaces and stored without rinsing. Thanks to tin fluoride, there is a decrease in the formation of organic acids by bacteria, difficulty in the regulation of intracellular metabolism in them, disruption of membrane transport and adhesion of microorganisms to the surface of the teeth.
Suppression of microflora
Another important approach in preventing the development of caries in young children is to prevent premature colonization of the child’s oral cavity with cariogenic microflora, and if different levels of its contamination are recorded, to suppress its activity.
The source of microbes for a child’s oral cavity is mothers or other adults caring for him. Dental restoration. treatment and prevention of periodontal diseases in combination with chemical suppression of pathogenic flora of the oral cavity in mothers helps prevent the development of caries in young children. The risk of vertical transmission of cariogenic microbes can be reduced through regular maternal use of chewing gum containing xylitol. Children whose mothers regularly used such chewing gum for 5 years had a decrease in S. mutans
and caries activity
Another way to reduce the number of microorganisms in the oral cavity is to use various forms of chlorhexidine (in the form of toothpastes, rinses, gels, varnishes). Their use is possible in parallel both in children and in their mothers. For example, use once a week for 12 weeks. 0.2% chlorhexidine-containing dentifrice gel in 10-month-old children resulted in a reduction of S. mutans
to zero level.
And in 3-year-old children with intact dentition and a high risk of developing caries, after 1.5 years of regular use (once for 3 consecutive days with an interval of 3 months), the same gel had a moderate inhibitory effect on S. mutans;
66.4% of children continued to maintain an intact bite.
When comparing the rate of decrease in the number of colonies of microorganisms from the use of chlorhexidine- and fluoride-containing gels, it turned out that the level of S. mutans
decreased significantly after treating teeth with a chlorhexidine-containing gel (after 4 weeks of regular coatings); when treating teeth with a fluoride-containing gel, this occurs only after 12 weeks.
It is also optimal to use chlorhexidine digluconate to suppress acidogenic microflora in the form of a 1-minute oral bath, coating the fissures of permanent molars in children of primary school age with Cervitec Plus varnish containing 1% chlorhexidine and thymol reduces the likelihood of developing fissure caries and leads to a decrease in S. mutans,
even after 3 months.
A highly effective result was obtained from the use of 10% povidone-iodine applied 2 times a month for 1 year to the intact teeth of children 12-19 months old who had a high risk of developing caries.
After 12 months 91% of children had no caries. Local application of agents with antimicrobial properties is quite promising for the stabilization and prevention of early caries .
⇐ Previous2Next ⇒
Basis of construction
The construction of the bite height is based on determining the distance between the two jaws in the position of maximum intercuspal closure of the teeth.
This indicator is of great importance in dental practice, since it allows one to determine the correct location of the elements of the dentofacial row.
A change in the physiological height of the bite as a result of the loss of some teeth or their displacement relative to the jaw line entails a change in the position of the main anatomical elements that surround the oral cavity.
In this situation, the patient is diagnosed with sunken lips, an increase in the depth of the nasolabial folds, a significant protrusion of the chin forward, and a decrease in the height of the lower sector of the face.
In addition to being aesthetically unattractive, this situation significantly complicates further orthodontic and orthopedic therapy.
IV PERIOD - from 3 to 6 years (the period of formed temporary occlusion)
Prevention of dental anomalies:
- plastic surgery of a shortened or improperly attached frenulum of the tongue
- complexes of therapeutic exercises to normalize lip closure, position of the lower jaw and tongue at rest and during functions
- combating sluggish chewing, avoiding eating hard foods, learning to swallow correctly
- learning the correct pronunciation of individual sounds (“r”, “l”, hissing)
- planned sanitation and hygiene of the oral cavity using special-purpose products
- monitoring the depth of the incisal overlap and the shape of the dental arches
- identification of postural disorders, flat feet, teaching correct body position while standing, sitting, lying, walking
- introduction to outdoor games
Reasons for the development of the anomaly
There are many reasons that influence the height of a person’s bite. Dentists name the following factors that contribute to reducing the distance between the jaws in occlusion:
- pathological abrasion of the tooth surface , accompanied by loss of its density and subsequent destruction of incisors and molars;
- bruxism or teeth grinding , which entails enamel deformation, subsidence of teeth and a decrease in central occlusion;
- uneven chewing load in certain areas of the jaw row, which often occurs when restoring teeth using a prosthetic bridge;
- loss of molars on one or both jaws;
- destruction and extraction of several teeth in combination with displacement of the remaining elements of the row relative to the central jaw line;
- metabolic disorders in the body , which entails a deficiency of calcium and phosphorus, which affects the strength of bone tissue and contributes to its atrophy;
- improperly manufactured prosthetic structures.
In order for prosthetic structures to be manufactured correctly, it is necessary to carry out a considerable number of measurements, one of which is considered to be carrying out all studies in a state of physiological rest of the patient’s maxillofacial apparatus.
How dental impressions are taken for prosthetics and orthodontic treatment.
Read here about the purpose of teeth filing.
PERIOD IX - from 21 to 40 years (active functions of the dental system)
Prevention and treatment of dental anomalies:
- regular sanitation of the oral cavity, compliance with hygiene rules using special-purpose products
- observation by a periodontist, treatment of periodontal diseases
- professional oral hygiene
- restoration of crowns of damaged teeth
- replacement of missing teeth using implantation and prosthetics
- removal of 3 molars
- selective grinding of teeth and elimination of traumatic occlusion
- achieving multiple contacts between teeth with various types of articulation and occlusion of the dentition
- prevention of diseases of the temporomandibular joints
- food hygiene
- elimination of calcium deficiency
- sports, fitness, swimming
- identification and elimination of risk factors
- fighting bad habits
- prevention of secondary dentofacial deformations
no images were found
Physiological rest
Dentists call the position of the upper and lower jaws relative to each other with maximum relaxation of the muscles of the maxillofacial apparatus physiological rest. Their retention is based on the anti-gravity reflex.
As a rule, in a state of relaxation, which is characteristic of the human oral cavity outside of eating and communicating, the teeth do not come into contact with their antagonists.
Dentists consider the distance between opposite jaw rows to be no more than 2-5 mm as a normal option.
Experts distinguish two variants of bite pathology, depending on the degree of its height:
- Overpriced. The cause of this phenomenon is an incorrectly designed prosthesis.
As a result of overbite, the antagonist teeth are constantly in contact, and the difference between the location of the teeth in central occlusion and at rest does not exceed 1-2 mm or is completely absent.
It is difficult for the patient to close his lips tightly, causing discomfort during communication. The danger of the pathology lies in systematic injury to the prosthetic bed, prolonged tension in the masticatory muscles, which can lead to damage to the joint. Understated. The cause of this occlusion pathology is increased wear of the tooth surface or an incorrectly fitted prosthetic structure.
Dentists diagnose underbite when the difference between the resting state and central occlusion is more than 3-4 mm. The patient's appearance changes significantly.
Concomitant pathologies
Malocclusion is formed due to a number of reasons, congenital or acquired. These include:
- insufficient calcium intake during fetal development;
- hereditary tendency to abrasion of enamel;
- chronic infections of ENT organs;
- bad habits (biting nails, thumb sucking, putting your hand under your chin).
Due to pathology, a person may develop health problems:
- Impaired functioning of the gastrointestinal tract. When digesting large pieces of food, the stomach experiences increased stress.
- Periodontal disease. It occurs due to unevenly distributed load on different parts of the jaw.
- Increased risk of enamel wear. Because of this, teeth are more susceptible to caries.
- Pathologies of the temporal joint , which are manifested by constant headaches.
- Injury to the soft tissues of the mouth. Because of this, wounds and ulcers appear on the surface of the mucous membranes.
- Speech dysfunction.
- Labored breathing.
An abnormal bite is the cause of an aesthetic defect. If the teeth are incorrectly positioned, the proportions of the face change and its symmetry is disrupted.
If a problem occurs, you must contact a specialist as early as possible to prevent complications from developing.
Measurement methods
Anatomical method
The use of this method of measuring bite height is aimed at identifying the physiological transformation of the lower part of the facial zone.
Calculation of central occlusion using this method is based on identifying features of facial anatomy.
A decrease in bite height is expressed in the following points:
- sunken lips;
- increasing the depth of nasolabial folds;
- moving the chin forward;
- reduction in the height of the lower part of the face.
When using the anatomical method, you need to pay attention to the following points:
- the lips should be mobile and in contact with each other along the entire length without effort;
- the functionality of the orbicularis oris muscle should be high;
- The elevation of the corners of the mouth and the severity of the nasolabial folds should be determined.
Experts in the field of dentistry note that this research method is quite subjective , so it is practically not used at present.
Information content of teleroentgenograms in orthodontics in lateral and direct projection.
This material is devoted to modern diagnostic methods in dentistry.
Anatomical and physiological
The anatomical and physiological method for determining the height of the bite is based on identifying the height of physiological rest.
The technique for performing the procedure is as follows:
- The dentist places two marks on the patient's skin - at the base of the nasal septum and in the central part of the chin.
- Next, the patient is asked to make a couple of swallowing movements or pronounce several phrases, the pronunciation of which involves the lips.
After completing these actions, the lower jaw row comes to a state of rest. At the same time, the lips touch each other without tension, without stretching or sinking, and the nasolabial folds are moderately visible.
- The dentist, using a special ruler with divisions, measures the distance between two points that were previously applied to the patient’s skin.
- Special templates with occlusal ridges are placed in the patient’s oral cavity, which must be lightly bitten.
- The specialist re-measures the distance between the points located on the nose and chin. The resulting indicator determines the occlusal height, which normally should be less than the previously determined height of physiological rest by 2-3 mm.
If, when determining the height of the bite, the occlusal height is equal to the indicator determined at rest, then the specialist concludes that the bite is elevated. Conversely, when the occlusal distance exceeds the resting height by more than 3-4 mm, this indicates an underbite.
After determining the bite index, the specialist removes or increases the height of the lower bite ridge until the occlusal height reaches the norm.
In this case, the dentist evaluates the condition of the tissues around the mouth. When the physiological occlusion is restored, the contours of the lower part of the face are normalized, the corners of the mouth are raised, and the nasolabial folds become less pronounced.
Planning for prosthetics
The manufacture and fixation of prosthetic structures for pathological bite heights have certain features and require careful planning and preparation.
Preparatory measures for prosthetics differ somewhat depending on the identified pathology of the relationship of the upper and lower jaw.
Thus, the main action in determining a low bite is the production of special aligners and bite plates, with the help of which complex orthodontic treatment is carried out.
These designs are made individually for each patient, taking into account the impressions of his oral cavity. The purpose of this procedure is to bring the occlusal height indicator to a state of physiological norm.
The duration of use of bite blocks and mouthguards depends on the severity of the pathology, as well as the anatomical features of the structure and functioning of the bone and muscle structures of the human oral cavity.
If a low bite is detected, the following preparatory measures for subsequent prosthetics can be used:
If it is not possible to correct the height of the bite using orthodontic devices, specialists resort to more radical methods, in particular surgical intervention.
In this case, the root system of one or more teeth is exposed and the gum tissue is given the required shape and relief.
The video provides additional information on the topic of the article.
What to do if the bite is formed incorrectly
If the problem has already appeared, the teeth are growing in the wrong position, the fangs protrude towards the cheeks, and the incisors are crowded, then you need to consult a dentist as soon as possible. Parents should understand that the sooner orthodontic treatment begins, the easier it will be. You should not think that over time the position of the jaw will correct and align on its own. Most often, this does not happen, and the child then suffers from aesthetic and physiological discomfort all his life. Therefore, the most correct option when developing a malocclusion would be to seek medical help.